Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Oxygen TherapyDocumento44 páginasOxygen TherapyChhabilal BastolaAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- CG en PDFDocumento335 páginasCG en PDFJessicaPaolaGutiérrezAranaAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- 7 TH Semester Dermatology LecturesDocumento44 páginas7 TH Semester Dermatology LecturesChhabilal BastolaAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Altered Sensorium and Care of Unconscious PatientsDocumento17 páginasAltered Sensorium and Care of Unconscious PatientsChhabilal BastolaAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- 7 TH Semester Anesthesia LecturesDocumento35 páginas7 TH Semester Anesthesia LecturesChhabilal BastolaAinda não há avaliações
- Opioids in AnaesthesiaDocumento28 páginasOpioids in AnaesthesiaChhabilal BastolaAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Investigations For Thrombotic Tendencies - Australian Prescriber PDFDocumento6 páginasInvestigations For Thrombotic Tendencies - Australian Prescriber PDFChhabilal BastolaAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Laboratory Diagnosis of Coagulation DisordersDocumento59 páginasLaboratory Diagnosis of Coagulation DisordersChhabilal BastolaAinda não há avaliações
- 42 Deep Thought On Life, The Universe, and EverythingDocumento195 páginas42 Deep Thought On Life, The Universe, and EverythingHenry Ford100% (3)
- Emergency Drug Doses - PBS Doctor's Bag Items - Australian PrescriberDocumento4 páginasEmergency Drug Doses - PBS Doctor's Bag Items - Australian PrescriberChhabilal BastolaAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Meningitis and Brain AbscessDocumento32 páginasMeningitis and Brain AbscessChhabilal BastolaAinda não há avaliações
- ChronicKidneyDisease IX Semseter MBBSDocumento38 páginasChronicKidneyDisease IX Semseter MBBSChhabilal BastolaAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
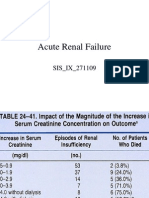
- Acute Renal FailureDocumento125 páginasAcute Renal FailureChhabilal BastolaAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Dental Anatomy For MBBSDocumento33 páginasDental Anatomy For MBBSChhabilal BastolaAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- ERC Guidelines 2005 Advanced Adult Life SupportDocumento48 páginasERC Guidelines 2005 Advanced Adult Life SupportJoãoBrasil100% (2)
- Resusgl 2010Documento157 páginasResusgl 2010Salman IslamAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Usmle LabsDocumento3 páginasUsmle LabsAdnan KhurshidAinda não há avaliações
- Wellness and Fitness Exercise ManualDocumento63 páginasWellness and Fitness Exercise ManualcienciaxAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Kumj-Guideline For AuthorsDocumento6 páginasKumj-Guideline For AuthorsChhabilal BastolaAinda não há avaliações
- UsmleDocumento58 páginasUsmleFaisal Chukwudera Adam100% (1)
- How - To - Read - Guitar TabDocumento29 páginasHow - To - Read - Guitar TabChhabilal Bastola100% (3)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Snake Bite ManagementDocumento49 páginasSnake Bite ManagementChhabilal BastolaAinda não há avaliações
- Step 3: Content Description and General InformationDocumento73 páginasStep 3: Content Description and General Informations1234321Ainda não há avaliações
- Lyrics and Chords From UltimateDocumento2 páginasLyrics and Chords From UltimateChhabilal BastolaAinda não há avaliações
- Top 100 QS World University Rankings For Medicine 2011 - Higher Education Network - Guardian ProfessionalDocumento5 páginasTop 100 QS World University Rankings For Medicine 2011 - Higher Education Network - Guardian ProfessionalChhabilal BastolaAinda não há avaliações
- 2010 Step 2 CKDocumento76 páginas2010 Step 2 CKandres ord100% (2)
- Im Yours Chords: by Jason MrazDocumento2 páginasIm Yours Chords: by Jason MrazChhabilal BastolaAinda não há avaliações
- LyricsDocumento2 páginasLyricsChhabilal BastolaAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Top 100 QS World University Rankings For Medicine 2011 - Higher Education Network - Guardian ProfessionalDocumento5 páginasTop 100 QS World University Rankings For Medicine 2011 - Higher Education Network - Guardian ProfessionalChhabilal BastolaAinda não há avaliações
- Pituitary Disorders (Final Draft)Documento17 páginasPituitary Disorders (Final Draft)Kiprono Keitany TimothyAinda não há avaliações
- Esophageal AtresiaDocumento9 páginasEsophageal AtresiaAnonymous 9xHTwHYAinda não há avaliações
- Master of Science in RadiodiagnosisDocumento73 páginasMaster of Science in RadiodiagnosisCwali MohamedAinda não há avaliações
- TNCC Study GuideDocumento6 páginasTNCC Study Guidekristinekat96% (24)
- Seminar: DiagnosisDocumento14 páginasSeminar: DiagnosisyenyenAinda não há avaliações
- Tumor Pituitari: Pembimbing: Ervita Yuda, DR., SPPD, M.Kes Davin Takaryanto, DRDocumento34 páginasTumor Pituitari: Pembimbing: Ervita Yuda, DR., SPPD, M.Kes Davin Takaryanto, DRDavin TakaryantoAinda não há avaliações
- Ez GuardDocumento18 páginasEz GuardAvaemmaAinda não há avaliações
- Ms Test-Questio 2Documento24 páginasMs Test-Questio 2Jackie AbarraAinda não há avaliações
- Asam PeroksideDocumento6 páginasAsam PeroksideAsa Étudier La-DienAinda não há avaliações
- Normal Respiratory Rate and Heart Rate in Children - UpToDateDocumento2 páginasNormal Respiratory Rate and Heart Rate in Children - UpToDateKrishn DsAinda não há avaliações
- Calcium Channel BlockersDocumento28 páginasCalcium Channel Blockershap hazardAinda não há avaliações
- Physical Assessment of Preeclamptic PatientDocumento3 páginasPhysical Assessment of Preeclamptic PatientAndreiAinda não há avaliações
- Olympus EndosDocumento9 páginasOlympus EndoshoneyworksAinda não há avaliações
- NCP MakingDocumento2 páginasNCP MakingMinakaAinda não há avaliações
- Assissting FNAB in The Liver Liver Biopsy Checklist FinalDocumento10 páginasAssissting FNAB in The Liver Liver Biopsy Checklist FinalCamille T. SanchezAinda não há avaliações
- Disorders of Skin in ChildrenDocumento47 páginasDisorders of Skin in Childrensmriti boraAinda não há avaliações
- Inst Branchwise Mdmsdiploma Adm 28072020Documento89 páginasInst Branchwise Mdmsdiploma Adm 28072020XAinda não há avaliações
- Case Study OsteomyelitisDocumento3 páginasCase Study OsteomyelitisFirsandiPrasastyaFikryGozaliAinda não há avaliações
- KAD Pada DM Tipe 1Documento56 páginasKAD Pada DM Tipe 1hilmiana putriAinda não há avaliações
- Open Jejunostomy: Steven J. Hughes, MD and A. James Moser, MDDocumento8 páginasOpen Jejunostomy: Steven J. Hughes, MD and A. James Moser, MDAndres BernalAinda não há avaliações
- HS FA Answer Key PDFDocumento4 páginasHS FA Answer Key PDFGent'Ainda não há avaliações
- Varicocele and Testicular PainDocumento7 páginasVaricocele and Testicular PainseptaayuAinda não há avaliações
- Rehabilitation After Plate Fixation of Upper and Lower Extremity FracturesDocumento6 páginasRehabilitation After Plate Fixation of Upper and Lower Extremity FractureswirasenaAinda não há avaliações
- Clinical Guidelines (Nursing) - Oxygen DeliveryDocumento16 páginasClinical Guidelines (Nursing) - Oxygen DeliveryPhan0% (1)
- 2012 Complete Board Questions PDFDocumento43 páginas2012 Complete Board Questions PDFbmhshAinda não há avaliações
- Heart Failure: Dr. Niva WDocumento32 páginasHeart Failure: Dr. Niva WNiva Wilujeng100% (1)
- Brugia MalayiDocumento4 páginasBrugia MalayiJericha IsidroAinda não há avaliações
- Week 10. COURSE TASK - Mrs. Clot's and Alexa's CaseDocumento1 páginaWeek 10. COURSE TASK - Mrs. Clot's and Alexa's CaseTerence SalamatAinda não há avaliações
- Ec/irbDocumento28 páginasEc/irbRachana ShettyAinda não há avaliações
- Parasitology TablesDocumento9 páginasParasitology Tables2013SecB92% (26)
- Proof of Heaven: A Neurosurgeon's Journey into the AfterlifeNo EverandProof of Heaven: A Neurosurgeon's Journey into the AfterlifeNota: 3.5 de 5 estrelas3.5/5 (165)
- Secrets of the Millionaire Mind: Mastering the Inner Game of WealthNo EverandSecrets of the Millionaire Mind: Mastering the Inner Game of WealthNota: 4.5 de 5 estrelas4.5/5 (197)
- The Game: Penetrating the Secret Society of Pickup ArtistsNo EverandThe Game: Penetrating the Secret Society of Pickup ArtistsNota: 4 de 5 estrelas4/5 (131)
- Hollywood & the Best of Los Angeles Travel GuideNo EverandHollywood & the Best of Los Angeles Travel GuideNota: 4.5 de 5 estrelas4.5/5 (2)