Você também pode gostar
- Opioids in AnaesthesiaDocumento28 páginasOpioids in AnaesthesiaChhabilal BastolaAinda não há avaliações
- Laboratory Diagnosis of Coagulation DisordersDocumento59 páginasLaboratory Diagnosis of Coagulation DisordersChhabilal BastolaAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- CG en PDFDocumento335 páginasCG en PDFJessicaPaolaGutiérrezAranaAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Oxygen TherapyDocumento44 páginasOxygen TherapyChhabilal BastolaAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Resusgl 2010Documento157 páginasResusgl 2010Salman IslamAinda não há avaliações
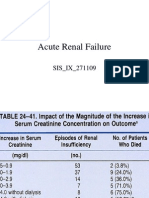
- Acute Renal FailureDocumento125 páginasAcute Renal FailureChhabilal BastolaAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Unconscious PatientDocumento19 páginasUnconscious PatientChhabilal BastolaAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Altered Sensorium and Care of Unconscious PatientsDocumento17 páginasAltered Sensorium and Care of Unconscious PatientsChhabilal BastolaAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- 7 TH Semester Anesthesia LecturesDocumento35 páginas7 TH Semester Anesthesia LecturesChhabilal BastolaAinda não há avaliações
- Meningitis and Brain AbscessDocumento32 páginasMeningitis and Brain AbscessChhabilal BastolaAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Emergency Drug Doses - PBS Doctor's Bag Items - Australian PrescriberDocumento4 páginasEmergency Drug Doses - PBS Doctor's Bag Items - Australian PrescriberChhabilal BastolaAinda não há avaliações
- Kumj-Guideline For AuthorsDocumento6 páginasKumj-Guideline For AuthorsChhabilal BastolaAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Investigations For Thrombotic Tendencies - Australian Prescriber PDFDocumento6 páginasInvestigations For Thrombotic Tendencies - Australian Prescriber PDFChhabilal BastolaAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Dental Anatomy For MBBSDocumento33 páginasDental Anatomy For MBBSChhabilal BastolaAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- ChronicKidneyDisease IX Semseter MBBSDocumento38 páginasChronicKidneyDisease IX Semseter MBBSChhabilal BastolaAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- ERC Guidelines 2005 Advanced Adult Life SupportDocumento48 páginasERC Guidelines 2005 Advanced Adult Life SupportJoãoBrasil100% (2)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- 42 Deep Thought On Life, The Universe, and EverythingDocumento195 páginas42 Deep Thought On Life, The Universe, and EverythingHenry Ford100% (3)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- Snake Bite ManagementDocumento49 páginasSnake Bite ManagementChhabilal BastolaAinda não há avaliações
- How - To - Read - Guitar TabDocumento29 páginasHow - To - Read - Guitar TabChhabilal Bastola100% (3)
- Step 3: Content Description and General InformationDocumento73 páginasStep 3: Content Description and General Informations1234321Ainda não há avaliações
- Usmle LabsDocumento3 páginasUsmle LabsAdnan KhurshidAinda não há avaliações
- Wellness and Fitness Exercise ManualDocumento63 páginasWellness and Fitness Exercise ManualcienciaxAinda não há avaliações
- UsmleDocumento58 páginasUsmleFaisal Chukwudera Adam100% (1)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- 2010 Step 2 CKDocumento76 páginas2010 Step 2 CKandres ord100% (2)
- Im Yours Chords: by Jason MrazDocumento2 páginasIm Yours Chords: by Jason MrazChhabilal BastolaAinda não há avaliações
- LyricsDocumento2 páginasLyricsChhabilal BastolaAinda não há avaliações
- Lyrics and Chords From UltimateDocumento2 páginasLyrics and Chords From UltimateChhabilal BastolaAinda não há avaliações
- Top 100 QS World University Rankings For Medicine 2011 - Higher Education Network - Guardian ProfessionalDocumento5 páginasTop 100 QS World University Rankings For Medicine 2011 - Higher Education Network - Guardian ProfessionalChhabilal BastolaAinda não há avaliações
- Top 100 QS World University Rankings For Medicine 2011 - Higher Education Network - Guardian ProfessionalDocumento5 páginasTop 100 QS World University Rankings For Medicine 2011 - Higher Education Network - Guardian ProfessionalChhabilal BastolaAinda não há avaliações
- Immune System - Answer KeyDocumento3 páginasImmune System - Answer Keyapi-250022577Ainda não há avaliações
- HRG-003 - The Genetics of Equine Coat ColorDocumento12 páginasHRG-003 - The Genetics of Equine Coat ColorJosefinaBravoAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Hillson Thyroid DisordersDocumento90 páginasHillson Thyroid DisordersGirish SubashAinda não há avaliações
- Removable Prosthodontics: Textbook ofDocumento13 páginasRemovable Prosthodontics: Textbook ofRico Anas0% (2)
- Pernicious Anemia: BSMT 3D Group 1 Paniza, Erika Joy Villanueva, Andrewarnold Yandan, CharisDocumento53 páginasPernicious Anemia: BSMT 3D Group 1 Paniza, Erika Joy Villanueva, Andrewarnold Yandan, CharisAndrew Arnold David VillanuevaAinda não há avaliações
- DeFronzo Et Al-2012-Diabetes, Obesity and MetabolismDocumento10 páginasDeFronzo Et Al-2012-Diabetes, Obesity and MetabolismlguerreroAinda não há avaliações
- Cardio Physiology FullDocumento11 páginasCardio Physiology FullSara Lee Wei LiAinda não há avaliações
- Single Remedy 3 Mark Rubrics in Kent's RepertoryDocumento27 páginasSingle Remedy 3 Mark Rubrics in Kent's RepertorymailbabuAinda não há avaliações
- USMLE Road Map ImmunologyDocumento242 páginasUSMLE Road Map ImmunologyFernanda Granillo100% (9)
- Development of The FaceDocumento76 páginasDevelopment of The Facedr parveen bathla100% (1)
- 37981-iUBT311 Treatment Evidence Form v2Documento5 páginas37981-iUBT311 Treatment Evidence Form v2Aline Brito Ferreira de CastroAinda não há avaliações
- Facebow Calliper ReviewDocumento5 páginasFacebow Calliper ReviewFaheemuddin Muhammad100% (3)
- Diagnosis and Treatment of Viral Encephalitis: ReviewDocumento10 páginasDiagnosis and Treatment of Viral Encephalitis: ReviewnataliaAinda não há avaliações
- Proceedings of The Workshop On Frozen Semen Production o 16 Janu001 PDFDocumento88 páginasProceedings of The Workshop On Frozen Semen Production o 16 Janu001 PDFAnil JindalAinda não há avaliações
- Alda Risma CaseDocumento14 páginasAlda Risma CaseAci LusianaAinda não há avaliações
- NCPDocumento3 páginasNCPchesca_paunganAinda não há avaliações
- 3-4. LM in Eng 5 Q3 Week 3-4Documento24 páginas3-4. LM in Eng 5 Q3 Week 3-4Bea DeLuis de TomasAinda não há avaliações
- Orthodontic Case PresentationDocumento21 páginasOrthodontic Case PresentationEman Nazzal100% (1)
- AMEBIASISDocumento19 páginasAMEBIASISDika Herza Pratama100% (1)
- PTP Guideline 2014Documento35 páginasPTP Guideline 2014mukeshkumar@ibasukkurAinda não há avaliações
- 2022PET JZ FIA VETCHECK Brochures Ver - JZDocumento12 páginas2022PET JZ FIA VETCHECK Brochures Ver - JZAsesoria TecnicaAinda não há avaliações
- Klasifikasi Lablab PurpureusDocumento1 páginaKlasifikasi Lablab PurpureusWinda AriniAinda não há avaliações
- Makeup Secrets RevealedDocumento25 páginasMakeup Secrets RevealedPrerna Gill100% (2)
- Sex Determination and Sex Chromosomes: Lecture Presentations by Cindy Malone California State University, NorthridgeDocumento53 páginasSex Determination and Sex Chromosomes: Lecture Presentations by Cindy Malone California State University, NorthridgeAudrey100% (1)
- Interceptive OrthodonticsDocumento38 páginasInterceptive OrthodonticsFinhas100% (5)
- FKTP Perujuk Dengan Diagnosa Non Spesialistik SD April 2015Documento21 páginasFKTP Perujuk Dengan Diagnosa Non Spesialistik SD April 2015wibiAinda não há avaliações
- Cell Sensitivity to RadiationDocumento18 páginasCell Sensitivity to RadiationLouella ArtatesAinda não há avaliações
- Labrador Retriever: Illustrated StandardDocumento14 páginasLabrador Retriever: Illustrated StandardFrancisco VilledaAinda não há avaliações
- Literature Review On Goat ProductionDocumento5 páginasLiterature Review On Goat Productionafmzmqwdglhzex100% (1)
- Hemomancy: The Arcane Arts of BloodDocumento12 páginasHemomancy: The Arcane Arts of BloodMathieu Bst-georges100% (1)
- Secrets of the Millionaire Mind: Mastering the Inner Game of WealthNo EverandSecrets of the Millionaire Mind: Mastering the Inner Game of WealthNota: 4.5 de 5 estrelas4.5/5 (197)
- Proof of Heaven: A Neurosurgeon's Journey into the AfterlifeNo EverandProof of Heaven: A Neurosurgeon's Journey into the AfterlifeNota: 3.5 de 5 estrelas3.5/5 (165)
- Coastal Alaska & the Inside Passage Adventure Travel GuideNo EverandCoastal Alaska & the Inside Passage Adventure Travel GuideAinda não há avaliações
- The Game: Penetrating the Secret Society of Pickup ArtistsNo EverandThe Game: Penetrating the Secret Society of Pickup ArtistsNota: 4 de 5 estrelas4/5 (131)