Você também pode gostar
- Hyperlipidemia 1Documento32 páginasHyperlipidemia 1Binita ShakyaAinda não há avaliações
- Treatment of Hyperlipidemias: Pharmacology TeamDocumento53 páginasTreatment of Hyperlipidemias: Pharmacology TeamZaina Masri100% (1)
- Drugs For HyperlipidemiaDocumento29 páginasDrugs For Hyperlipidemiasultan khabeebAinda não há avaliações
- Inborn Errors of Lipid MetabolismDocumento41 páginasInborn Errors of Lipid MetabolismWalterAinda não há avaliações
- Dyslipidemia: Hisham Aljadhey, Pharmd, PHDDocumento55 páginasDyslipidemia: Hisham Aljadhey, Pharmd, PHDRany Waisya0% (1)
- Shelly HyperlipidemiaDocumento22 páginasShelly Hyperlipidemiaale marilAinda não há avaliações
- Penatalaksanaan Dislipidemia Statin Sebagai Salah Satu Modalitas TerapiDocumento21 páginasPenatalaksanaan Dislipidemia Statin Sebagai Salah Satu Modalitas TerapiDissa Naratania HantraAinda não há avaliações
- Lipid Biokimia Semester 2Documento93 páginasLipid Biokimia Semester 2Anonymous oyAUZoCeyAinda não há avaliações
- Lecture 11 Atherosclerosis N Fatty LiverDocumento24 páginasLecture 11 Atherosclerosis N Fatty Livernironkushbhuyan2002Ainda não há avaliações
- Anti - HyperlipidemiaDocumento18 páginasAnti - HyperlipidemiaZakarie Abdullahi Hussein100% (1)
- Dyslipidemia overviewDocumento90 páginasDyslipidemia overviewElena EllaAinda não há avaliações
- Dyslipidemia 2008Documento80 páginasDyslipidemia 2008Pucca' JernyAinda não há avaliações
- AtherosclerosisDocumento29 páginasAtherosclerosisneeraj banaAinda não há avaliações
- 14 DyslipidemiaDocumento45 páginas14 DyslipidemiaSaniAinda não há avaliações
- HyperlipidemiaDocumento22 páginasHyperlipidemiamaritzaAinda não há avaliações
- Guide to Hyperlipidemia (39Documento22 páginasGuide to Hyperlipidemia (39Febrina SusilawatiAinda não há avaliações
- DyslipidemiaDocumento44 páginasDyslipidemiaenri100% (1)
- Guide to Hyperlipidemia (39Documento22 páginasGuide to Hyperlipidemia (39Faisal AhmedAinda não há avaliações
- Guide to Hyperlipidemia (39Documento22 páginasGuide to Hyperlipidemia (39Ritha WidyaAinda não há avaliações
- Nutrition in Cardiovasular DiseaseDocumento62 páginasNutrition in Cardiovasular DiseaseMalisa Fitri UmarAinda não há avaliações
- Kuliah Dislipidemia UpdateDocumento44 páginasKuliah Dislipidemia UpdateYudy Hardiyansah100% (1)
- Hypolipidaemic Drugs: by Praveen Kumar Dixit Asst - Professor KIET School of PharmacyDocumento36 páginasHypolipidaemic Drugs: by Praveen Kumar Dixit Asst - Professor KIET School of Pharmacybhanu pratapAinda não há avaliações
- LipidDocumento31 páginasLipidahmed abd elazizAinda não há avaliações
- DyslipidaemiaDocumento34 páginasDyslipidaemiaMusfique RashidAinda não há avaliações
- Hyperlipidemia: Center of Post Graduate Studies in Family MedicineDocumento85 páginasHyperlipidemia: Center of Post Graduate Studies in Family MedicineShimelis MekitAinda não há avaliações
- Understanding Cholesterol Levels and Risks: A Guide to Lipid ProfilesDocumento48 páginasUnderstanding Cholesterol Levels and Risks: A Guide to Lipid ProfilesAnonymous o3Q3QXEAinda não há avaliações
- Dyslipidemia(1)Documento55 páginasDyslipidemia(1)earldioborrinagaAinda não há avaliações
- Drug Treatment of Hyperlipidemia: Philip Marcus, MD MPHDocumento56 páginasDrug Treatment of Hyperlipidemia: Philip Marcus, MD MPHVictor EkutaAinda não há avaliações
- Lipid Lowering Drugs True-1Documento51 páginasLipid Lowering Drugs True-1wissam salimAinda não há avaliações
- Lipoprotein Tests: Cholesterol (140-199 MG/DL)Documento3 páginasLipoprotein Tests: Cholesterol (140-199 MG/DL)imperiouxxAinda não há avaliações
- Dyslipidemia Harper CHODocumento37 páginasDyslipidemia Harper CHOC Hendra WijayaAinda não há avaliações
- 23 HyperlipidemiaDocumento85 páginas23 HyperlipidemiaIhab MoustafaAinda não há avaliações
- Management of HyperlipidemiaDocumento39 páginasManagement of HyperlipidemiaRajgopal100% (2)
- Medical Nutrition Therapy in Cardiovascular DiseaseDocumento93 páginasMedical Nutrition Therapy in Cardiovascular DiseasesariAinda não há avaliações
- Atherosclerosis, Dyslipidaemia and Diabetes SlidesDocumento83 páginasAtherosclerosis, Dyslipidaemia and Diabetes SlidesTatiana GobjilăAinda não há avaliações
- Cardiovascular Diseases and Hyperlipidemias: Continuing.Documento19 páginasCardiovascular Diseases and Hyperlipidemias: Continuing.Zai ZaiAinda não há avaliações
- Hypolipidemic Drugs PharmdDocumento38 páginasHypolipidemic Drugs Pharmddarlington D. y ayimAinda não há avaliações
- Lipid Profile L - DeterminatinDocumento33 páginasLipid Profile L - DeterminatinaliAinda não há avaliações
- Mbs127 Slide DislipidemiaDocumento45 páginasMbs127 Slide DislipidemiaDaru KristiyonoAinda não há avaliações
- CC1 Intro To Lipids 2016Documento60 páginasCC1 Intro To Lipids 2016Patrisha BuanAinda não há avaliações
- Antihyperlipidemic Agents: Statins and FibratesDocumento79 páginasAntihyperlipidemic Agents: Statins and FibratesKishori Kedia100% (1)
- Lecture Anti Hyperlipidemic DrugsDocumento21 páginasLecture Anti Hyperlipidemic DrugsNowfal Hasan SiamAinda não há avaliações
- Hypolipidemic AgentsDocumento39 páginasHypolipidemic AgentsAC ACAinda não há avaliações
- LipidsDocumento26 páginasLipidsparneetkaurbediAinda não há avaliações
- HYPERLIPIDEMIADocumento33 páginasHYPERLIPIDEMIAatiqullah tarmiziAinda não há avaliações
- Med 4 Lipedemias and Ischemic Heart DiseaseDocumento47 páginasMed 4 Lipedemias and Ischemic Heart DiseaseNathanAinda não há avaliações
- Hypolipidaemic DrugsDocumento6 páginasHypolipidaemic DrugsShamla HarisAinda não há avaliações
- Fatty Acids Vary in ShapeDocumento30 páginasFatty Acids Vary in ShapeVy NguyenAinda não há avaliações
- Dr. Drg. Nur Permatasari, MS. Dr. Dian Nugrahenny, M.BiomedDocumento24 páginasDr. Drg. Nur Permatasari, MS. Dr. Dian Nugrahenny, M.BiomedTutde SedanaAinda não há avaliações
- Chapter 26Documento33 páginasChapter 26raul sinatoAinda não há avaliações
- Hyperlipedemia PPDocumento51 páginasHyperlipedemia PPrabarAinda não há avaliações
- Hyprlipdemia 2020 4th EditionDocumento24 páginasHyprlipdemia 2020 4th EditionLillian KrazemAinda não há avaliações
- Lipid Lowering AngentDocumento22 páginasLipid Lowering AngentDave BraveAinda não há avaliações
- Hypolipidemic DrugsDocumento47 páginasHypolipidemic DrugsDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- Dyslipidemia Risk FactorDocumento8 páginasDyslipidemia Risk FactoragathageraldyneAinda não há avaliações
- Managing Hyperlipidemia in a 56-Year-Old Male PatientDocumento11 páginasManaging Hyperlipidemia in a 56-Year-Old Male Patientabdul basithAinda não há avaliações
- Measurement of serum lipids profile (Lipids Panel or Coronary Risk PanelDocumento26 páginasMeasurement of serum lipids profile (Lipids Panel or Coronary Risk Panelزين العابدين محمد عويشAinda não há avaliações
- 8 - Lipoprotéines 3Documento21 páginas8 - Lipoprotéines 3nour achkarAinda não há avaliações
- Fast Facts: Hyperlipidemia: Bringing clarity to lipid managementNo EverandFast Facts: Hyperlipidemia: Bringing clarity to lipid managementAinda não há avaliações
- Fast Facts: Familial Chylomicronemia Syndrome: Raising awareness of a rare genetic diseaseNo EverandFast Facts: Familial Chylomicronemia Syndrome: Raising awareness of a rare genetic diseaseAinda não há avaliações
- Clin Diabetes 2006 Kruse 91 3Documento3 páginasClin Diabetes 2006 Kruse 91 3Natasya Ryani PurbaAinda não há avaliações
- Unlock Bootloader and Flash Recovery on Qualcomm DevicesDocumento1 páginaUnlock Bootloader and Flash Recovery on Qualcomm DevicesAnonymous 1jCVqQuAinda não há avaliações
- HiperkolesterolDocumento2 páginasHiperkolesterolAnonymous 1jCVqQuAinda não há avaliações
- HiperkolesterolDocumento60 páginasHiperkolesterolAnonymous 1jCVqQuAinda não há avaliações
- Plasma Homocysteine and Total Thiol Content in Patients With Exudative Age-Related Macular DegenerationDocumento5 páginasPlasma Homocysteine and Total Thiol Content in Patients With Exudative Age-Related Macular DegenerationAnonymous 1jCVqQuAinda não há avaliações
- Lesson 5 Investigate Conditions Needed For GerminationDocumento12 páginasLesson 5 Investigate Conditions Needed For GerminationJohany Gaona CruzAinda não há avaliações
- Sensation As If by Roberts PDFDocumento369 páginasSensation As If by Roberts PDFNauman Khan100% (1)
- QB For HMTDocumento11 páginasQB For HMTsmg26thmayAinda não há avaliações
- Holistic NursingDocumento7 páginasHolistic NursingSharmila Laxman DakeAinda não há avaliações
- Death Certificate: Shaheed Monsur Ali Medical College HospitalDocumento3 páginasDeath Certificate: Shaheed Monsur Ali Medical College HospitalBokul80% (5)
- Ulta Beauty Hiring AgeDocumento3 páginasUlta Beauty Hiring AgeShweta RachaelAinda não há avaliações
- Radio WavesDocumento17 páginasRadio WavesStuart Yong100% (1)
- Uco Bank Final (Simple Charts)Documento40 páginasUco Bank Final (Simple Charts)gopal8726Ainda não há avaliações
- Lab Manual - General Chemistry (Spring 2019)Documento83 páginasLab Manual - General Chemistry (Spring 2019)jinri sandeulAinda não há avaliações
- Forming Project ReportDocumento9 páginasForming Project ReportMayur ShindeAinda não há avaliações
- All India Test Series (2023-24)Documento22 páginasAll India Test Series (2023-24)Anil KumarAinda não há avaliações
- The Political Ecology of Food and AgricultureDocumento15 páginasThe Political Ecology of Food and AgricultureMitchAinda não há avaliações
- Rock CycleDocumento30 páginasRock CycleDenny PrawiraAinda não há avaliações
- Water Plant SOPDocumento6 páginasWater Plant SOPIndrie AgustinaAinda não há avaliações
- GLIMPSES - A Compilation of Uncensored Real Life Experiences With Mental Illness 30-07-11Documento329 páginasGLIMPSES - A Compilation of Uncensored Real Life Experiences With Mental Illness 30-07-11kimbakicks0% (1)
- Thermocold AWC PROZONE Tech PDFDocumento44 páginasThermocold AWC PROZONE Tech PDFAlexAinda não há avaliações
- Hawaii Hotel Performance by WeekDocumento1 páginaHawaii Hotel Performance by WeekHonolulu Star-AdvertiserAinda não há avaliações
- PME4 KeyDocumento2 páginasPME4 KeyyazicigaamzeAinda não há avaliações
- Human Resource Manab Gement 1 ModuleDocumento75 páginasHuman Resource Manab Gement 1 ModuleNelly ChiyanzuAinda não há avaliações
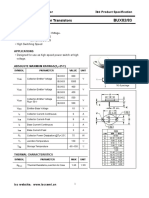
- Isc BUX82/83: Isc Silicon NPN Power TransistorsDocumento2 páginasIsc BUX82/83: Isc Silicon NPN Power TransistorsCarlos HCAinda não há avaliações
- Menstrual Hygiene PDFDocumento8 páginasMenstrual Hygiene PDFFarha AamirAinda não há avaliações
- IATA 04th Edition Cabin Operations Safety Best Practices GuideDocumento260 páginasIATA 04th Edition Cabin Operations Safety Best Practices GuideMakoto Ito100% (1)
- Disjointed.S01E03.720p.webrip.x264 STRiFE (Ettv) .SRTDocumento32 páginasDisjointed.S01E03.720p.webrip.x264 STRiFE (Ettv) .SRTArthur CarvalhoAinda não há avaliações
- Eastern RlyDocumento25 páginasEastern Rlyshivam.jhawar95Ainda não há avaliações
- Brake Accumulator Test and ChargeDocumento8 páginasBrake Accumulator Test and ChargeBarzola Soto Omar100% (1)
- Top 10 Credit Rating Agencies in WorldDocumento3 páginasTop 10 Credit Rating Agencies in Worldvmktpt100% (4)
- Life Skills Unit PlanDocumento15 páginasLife Skills Unit PlanLindy McBratneyAinda não há avaliações
- TV Commercials Depicting MothersDocumento2 páginasTV Commercials Depicting MothersClarence TumabiaoAinda não há avaliações
- American Institute of Timber Construction: AITC 405-2005Documento8 páginasAmerican Institute of Timber Construction: AITC 405-2005jerchiAinda não há avaliações
- Test - Ans SEAFOOD COOKERY 10Documento7 páginasTest - Ans SEAFOOD COOKERY 10EVANGELINE VILLASICAAinda não há avaliações