Você também pode gostar
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderNo EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderAinda não há avaliações
- Journal Club of Gastroentrology: Acute PancreatitisDocumento45 páginasJournal Club of Gastroentrology: Acute PancreatitisSyed Irfan ArifAinda não há avaliações
- Hypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionNo EverandHypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionAinda não há avaliações
- Unmet Needs in Diabetes: Present and Future From Clinical PracticeDocumento53 páginasUnmet Needs in Diabetes: Present and Future From Clinical PracticescribdAinda não há avaliações
- Prediabetes: A Fundamental Text: Pathophysiology, Complications, Management & ReversalNo EverandPrediabetes: A Fundamental Text: Pathophysiology, Complications, Management & ReversalAinda não há avaliações
- Acp Sglt2 Slidecast 220Documento169 páginasAcp Sglt2 Slidecast 220charanmann9165Ainda não há avaliações
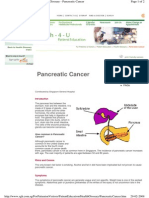
- Pancreatic CancerDocumento4 páginasPancreatic Cancersdf100% (1)
- Management of Liver CirrhosisDocumento7 páginasManagement of Liver Cirrhosispet_trinAinda não há avaliações
- Weight Loss Drug Cutting Risk of Heart AttackDocumento12 páginasWeight Loss Drug Cutting Risk of Heart AttackWKYC.comAinda não há avaliações
- Cleveland Clinic Journal of Medicine 2013 BARON 354 9Documento6 páginasCleveland Clinic Journal of Medicine 2013 BARON 354 9Stephanie PlascenciaAinda não há avaliações
- Compilation Of Patie…: Установите Google Документы!Documento1 páginaCompilation Of Patie…: Установите Google Документы!UpsetAinda não há avaliações
- NON Communicable DiseasesDocumento45 páginasNON Communicable DiseaseshemihemaAinda não há avaliações
- Effect of StatinDocumento26 páginasEffect of StatinLaluMuhammadSabarSetiawanAinda não há avaliações
- Chronic Kidney DiseaseDocumento39 páginasChronic Kidney DiseaseGumarbio Setiadi Zakaria100% (1)
- Crohns DiseaseDocumento72 páginasCrohns Diseasea1savedAinda não há avaliações
- Semaglutide and Cardiovascular Outcomes in Obesity Without DiabetesDocumento12 páginasSemaglutide and Cardiovascular Outcomes in Obesity Without Diabetesmengyanli.528Ainda não há avaliações
- In The Clinic - Acute PancreatitisDocumento16 páginasIn The Clinic - Acute PancreatitisSurapon Nochaiwong100% (1)
- The Influence of Metformin in The Etiology of Selected CancersDocumento7 páginasThe Influence of Metformin in The Etiology of Selected CancersMuhammad Reza IrzantoAinda não há avaliações
- 2012 Best Parctice Medical O Grady TH en FHADocumento7 páginas2012 Best Parctice Medical O Grady TH en FHASol Del Mar SarmientoAinda não há avaliações
- Non-Alcoholic Fatty Liver Disease in Patients With Type 2 - Tuong, Tran Thi Khanh Tran, Dang Khoa Phu, Pham Quang - Diagnostics, #3, 10, PagesDocumento11 páginasNon-Alcoholic Fatty Liver Disease in Patients With Type 2 - Tuong, Tran Thi Khanh Tran, Dang Khoa Phu, Pham Quang - Diagnostics, #3, 10, PagesLigia AbdalaAinda não há avaliações
- Registrar Teaching July 2007 Paul FrankishDocumento42 páginasRegistrar Teaching July 2007 Paul FrankishdaaaniiisAinda não há avaliações
- Journal SirosisDocumento9 páginasJournal SirosissarahAinda não há avaliações
- DD Metabolic SyndromeDocumento5 páginasDD Metabolic SyndromeEluAinda não há avaliações
- Bariatric Surgery AlokDocumento75 páginasBariatric Surgery AlokAlok BhallaAinda não há avaliações
- Common Renal DiseasesDocumento59 páginasCommon Renal DiseasesBegashawAinda não há avaliações
- Diabetes PregnancyDocumento65 páginasDiabetes PregnancyJohn Christopher LucesAinda não há avaliações
- Im Finals PDFDocumento49 páginasIm Finals PDFmarielleaudreeyAinda não há avaliações
- HTTPDocumento65 páginasHTTPAndreea SlabuAinda não há avaliações
- Acute Pancreatitis: in The ClinicDocumento16 páginasAcute Pancreatitis: in The ClinicdeltanueveAinda não há avaliações
- Diagnosis Kanker Pankreas PDFDocumento7 páginasDiagnosis Kanker Pankreas PDFAgustinus FatollaAinda não há avaliações
- Diabetes Update: Facts, Trends and ObservationsDocumento28 páginasDiabetes Update: Facts, Trends and ObservationsPilar Victoria Arrieta VegaAinda não há avaliações
- Acute Pancreatitis: Department of Critical Care Medicine King Saud Medical City Riyadh, Saudi ArabiaDocumento29 páginasAcute Pancreatitis: Department of Critical Care Medicine King Saud Medical City Riyadh, Saudi ArabiaONe's IwanAinda não há avaliações
- Polypharmacy in The Aging Patient A Review of Glycemic Control in Older Adults With Type 2 DiabetesDocumento12 páginasPolypharmacy in The Aging Patient A Review of Glycemic Control in Older Adults With Type 2 Diabetesapi-311409998Ainda não há avaliações
- CPG Management of Chronic Kidney Disease in Adults June 2011Documento47 páginasCPG Management of Chronic Kidney Disease in Adults June 2011Kokoland KukusAinda não há avaliações
- Endoscopy in The ElderlyDocumento7 páginasEndoscopy in The ElderlyFebyan AbotAinda não há avaliações
- Evaluation of Diabetes Mellitus Type 2 Effects On Kidney FunctionDocumento7 páginasEvaluation of Diabetes Mellitus Type 2 Effects On Kidney FunctionMediterr J Pharm Pharm SciAinda não há avaliações
- Management of Diabetes Mellitus in Patients With Chronic Kidney DiseaseDocumento9 páginasManagement of Diabetes Mellitus in Patients With Chronic Kidney DiseasezakyAinda não há avaliações
- Ulcerative Colitis Brochure PDFDocumento2 páginasUlcerative Colitis Brochure PDFicoanamareAinda não há avaliações
- Pathology of Type 2 DiabetesDocumento4 páginasPathology of Type 2 DiabetesJenny SembranoAinda não há avaliações
- Update On: Diabetes MellitusDocumento37 páginasUpdate On: Diabetes MellitusDr. Mamunul Abedin100% (1)
- Mingrone 2015Documento10 páginasMingrone 2015Ana GomezAinda não há avaliações
- Imunologi - Bella Suci Ramadhani - 42118005 - Review 1Documento13 páginasImunologi - Bella Suci Ramadhani - 42118005 - Review 1BellaAinda não há avaliações
- Reduction of Plasma Triglycerides by Diet in Subjects With Chronic Renal FailureDocumento15 páginasReduction of Plasma Triglycerides by Diet in Subjects With Chronic Renal FailureDina sayunaAinda não há avaliações
- Diabetic Nephropathy-The Family Physician's RoleDocumento7 páginasDiabetic Nephropathy-The Family Physician's RoleFaryalBalochAinda não há avaliações
- Diretrizes de Prática Clínica para o Tratamento de HipertrigliceriemiaDocumento24 páginasDiretrizes de Prática Clínica para o Tratamento de Hipertrigliceriemiaqmatheusq wsantoswAinda não há avaliações
- WHS PR Symposium - Non-Alcoholic Fatty Liver DiseaseDocumento63 páginasWHS PR Symposium - Non-Alcoholic Fatty Liver DiseaseWomen's Health SocietyAinda não há avaliações
- Vergara ReadingDocumento30 páginasVergara ReadingJan Leslie VergaraAinda não há avaliações
- Management of Lifestyle Factors in Individuals With Cirrhosis: A Pragmatic ReviewDocumento9 páginasManagement of Lifestyle Factors in Individuals With Cirrhosis: A Pragmatic ReviewsavitageraAinda não há avaliações
- Insulin Management in HospitalDocumento8 páginasInsulin Management in HospitalHannahAinda não há avaliações
- Kjjhuhyhhhhhhtttdddhhju 775433Documento4 páginasKjjhuhyhhhhhhtttdddhhju 775433dorinelAinda não há avaliações
- Diabetology & Metabolic Syndrome: Post-Transplant Diabetes MellitusDocumento4 páginasDiabetology & Metabolic Syndrome: Post-Transplant Diabetes MellitusVmiguel LcastilloAinda não há avaliações
- Pancreatitis Aguda para Emergencia PDFDocumento11 páginasPancreatitis Aguda para Emergencia PDFJudithzaloAinda não há avaliações
- Tuberculosis in Liver Cirrhosis: Rajesh Upadhyay, Aesha SinghDocumento3 páginasTuberculosis in Liver Cirrhosis: Rajesh Upadhyay, Aesha SinghAnastasia Lilian SuryajayaAinda não há avaliações
- Journal Case Report GiziDocumento5 páginasJournal Case Report GiziKeysha AbigailAinda não há avaliações
- Dr. S.P. Hewawasam (MD) Consultant Gastroenterologist/Senior Lecturer in PhysiologyDocumento33 páginasDr. S.P. Hewawasam (MD) Consultant Gastroenterologist/Senior Lecturer in PhysiologyAjung SatriadiAinda não há avaliações
- Health GuideDocumento2 páginasHealth Guidenktiah1207Ainda não há avaliações
- 26 Srinivasarao EtalDocumento7 páginas26 Srinivasarao EtaleditorijmrhsAinda não há avaliações
- GTG 33 Pcos 2014Documento15 páginasGTG 33 Pcos 2014Juan SetiajiAinda não há avaliações
- Lu 2014Documento6 páginasLu 2014Yanet FrancoAinda não há avaliações
- Guia para El MedicoDocumento6 páginasGuia para El MedicoJuan Sebastian OrdoñezAinda não há avaliações
- Biological WeaponsDocumento29 páginasBiological WeaponsSaad Motawéa100% (1)
- Outbreak Investigation Monday's ExerciseDocumento5 páginasOutbreak Investigation Monday's ExerciseSaad MotawéaAinda não há avaliações
- Giardia BenchaidDocumento2 páginasGiardia BenchaidSaad MotawéaAinda não há avaliações
- The Bizarre Claims of Hulda ClarkDocumento16 páginasThe Bizarre Claims of Hulda ClarkSaad Motawéa100% (1)
- Paraneoplastic SyndromeDocumento1 páginaParaneoplastic SyndromeSaad MotawéaAinda não há avaliações
- Pathogenomic Research in Hungary Present Stage and PerspectivesDocumento11 páginasPathogenomic Research in Hungary Present Stage and PerspectivesSaad MotawéaAinda não há avaliações
- 20 - Outbreak Investigation ReportDocumento26 páginas20 - Outbreak Investigation ReportSaad Motawéa50% (2)
- Supportive SupervisionDocumento21 páginasSupportive SupervisionSaad MotawéaAinda não há avaliações
- Case 2Documento20 páginasCase 2Saad MotawéaAinda não há avaliações
- Hexamine Fuel TabletDocumento4 páginasHexamine Fuel TabletSaad MotawéaAinda não há avaliações
- Immunisation - A Public Health Issue: Judith Moreton Programme ManagerDocumento15 páginasImmunisation - A Public Health Issue: Judith Moreton Programme ManagerSaad MotawéaAinda não há avaliações
- New York University School of Medicine Meeting of The Curriculum CommitteeDocumento2 páginasNew York University School of Medicine Meeting of The Curriculum CommitteeSaad MotawéaAinda não há avaliações
- S P - O F: Yllabus RE Rder ORMDocumento1 páginaS P - O F: Yllabus RE Rder ORMSaad MotawéaAinda não há avaliações
- Communicable Disease Epidemiology & Public Health Surveillance: An OverviewDocumento46 páginasCommunicable Disease Epidemiology & Public Health Surveillance: An OverviewSaad MotawéaAinda não há avaliações
- Hepatitis CDocumento86 páginasHepatitis CSaad Motawéa100% (1)
- Epidemiological Researches in Egypt: DR - Abdelnasser Mohammed AhmedDocumento21 páginasEpidemiological Researches in Egypt: DR - Abdelnasser Mohammed AhmedSaad MotawéaAinda não há avaliações
- 381 PDFDocumento7 páginas381 PDFSaad MotawéaAinda não há avaliações
- Hepatitis C Primer For HIV Care ProvidersDocumento26 páginasHepatitis C Primer For HIV Care ProvidersSaad MotawéaAinda não há avaliações
- Viral Hepatitis: Navy Environmental and Preventive Medicine Unit No. FiveDocumento57 páginasViral Hepatitis: Navy Environmental and Preventive Medicine Unit No. FiveSaad MotawéaAinda não há avaliações
- Tattoos Body PiercingsDocumento17 páginasTattoos Body PiercingsSaad MotawéaAinda não há avaliações
- Foot and Mouth Disease: Trina Johnson, Cari Ostrom, Carolyn Ritter, Craig Spray, and Lindsay WilsonDocumento25 páginasFoot and Mouth Disease: Trina Johnson, Cari Ostrom, Carolyn Ritter, Craig Spray, and Lindsay WilsonSaad MotawéaAinda não há avaliações
- Benha University Hospital, Egypt: Delta (Mansura) & Benha Fertility CentersDocumento55 páginasBenha University Hospital, Egypt: Delta (Mansura) & Benha Fertility CentersSaad MotawéaAinda não há avaliações
- Understanding FMDDocumento23 páginasUnderstanding FMDSaad MotawéaAinda não há avaliações
- Health Care Worker Health and Safety:: Preventing Needlestick Injury and Occupational Exposure To Bloodborne PathogensDocumento23 páginasHealth Care Worker Health and Safety:: Preventing Needlestick Injury and Occupational Exposure To Bloodborne PathogensSaad MotawéaAinda não há avaliações