Você também pode gostar
- Types of Surgical SuturesDocumento3 páginasTypes of Surgical Suturesruby cubionaAinda não há avaliações
- Suturing TechniqueDocumento13 páginasSuturing Techniquemannypot100% (1)
- Presentation1 HerniaDocumento12 páginasPresentation1 Herniatiwwiyeni16Ainda não há avaliações
- Inguinal HerniaDocumento29 páginasInguinal HerniaEzekiel Arteta100% (1)
- SuturingDocumento35 páginasSuturingAstuti Dwi WardaniAinda não há avaliações
- Cattle Uterine ProlapseDocumento3 páginasCattle Uterine ProlapseElena M. TilibaşaAinda não há avaliações
- Surgical NeedleDocumento11 páginasSurgical NeedleRicha RohillaAinda não há avaliações
- Basic Surgical Skills: Karthik.P JR Surgery Unit Iii AiimsDocumento40 páginasBasic Surgical Skills: Karthik.P JR Surgery Unit Iii AiimsbestsurgAinda não há avaliações
- Inguinal Hernia Surgery OverviewDocumento15 páginasInguinal Hernia Surgery OverviewWarda BajwaAinda não há avaliações
- Surgical Sutures From MbbsbasicDocumento55 páginasSurgical Sutures From Mbbsbasicbasic100% (5)
- Preecha's Technique MtF. (The Pioneer in Sex Reassignment Surgery, Thailand) - 1Documento7 páginasPreecha's Technique MtF. (The Pioneer in Sex Reassignment Surgery, Thailand) - 1VeroniqueAinda não há avaliações
- Chapter 55 - Pelvic Trauma Episode OverviewDocumento8 páginasChapter 55 - Pelvic Trauma Episode OverviewKadek Adi WigunaAinda não há avaliações
- Basic Wound Closure and Knot TyingDocumento26 páginasBasic Wound Closure and Knot TyingvaskemedAinda não há avaliações
- Management of Acute and Chronic Retention in MenDocumento52 páginasManagement of Acute and Chronic Retention in MenSri HariAinda não há avaliações
- Carcinoma Penis Management: Dr. Lilamani Rajthala MS Resident Moderator: Dr. Samir ShresthaDocumento63 páginasCarcinoma Penis Management: Dr. Lilamani Rajthala MS Resident Moderator: Dr. Samir ShresthaBibek GhimireAinda não há avaliações
- Principles of Abdominal Wall Closure - UpToDateDocumento32 páginasPrinciples of Abdominal Wall Closure - UpToDatesteve inga pomaAinda não há avaliações
- Man Age Men T of CancerDocumento14 páginasMan Age Men T of CancerKoRnflakesAinda não há avaliações
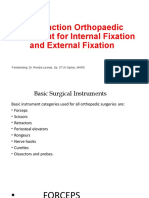
- Instrument TutorialDocumento114 páginasInstrument TutorialdwiswarapAinda não há avaliações
- SuturesDocumento30 páginasSuturesflori.bAinda não há avaliações
- Assessing AbdomenDocumento115 páginasAssessing AbdomenKris TinaAinda não há avaliações
- GenioplastyDocumento11 páginasGenioplastyMohamed El-shorbagyAinda não há avaliações
- Examination of Chronic AbdomenDocumento43 páginasExamination of Chronic AbdomendrrajeshpsmsAinda não há avaliações
- Suture LectureDocumento42 páginasSuture LectureAniz RataniAinda não há avaliações
- Guidelines For Therapeutic VenesectionDocumento2 páginasGuidelines For Therapeutic VenesectionDon Sudheera Dulan Abeysekara100% (1)
- Diagnosis and Classification of Urethral InjuriesDocumento13 páginasDiagnosis and Classification of Urethral Injuriesleo100% (2)
- CO2 Fractional Vaginal Tightenning Laser User's ManualDocumento25 páginasCO2 Fractional Vaginal Tightenning Laser User's ManualJorge CoboAinda não há avaliações
- PT Journal Musclel ActivityDocumento8 páginasPT Journal Musclel ActivityKarthigaMurugesanAinda não há avaliações
- Guidelines For Management of Head InjuryDocumento18 páginasGuidelines For Management of Head InjuryChellamani UmakanthanAinda não há avaliações
- Aesthetic, Breast 2001 PDFDocumento124 páginasAesthetic, Breast 2001 PDFAhmed AttiaAinda não há avaliações
- Amputation of The Penis: A.Venugopalan PG 212 LAS. 164Documento14 páginasAmputation of The Penis: A.Venugopalan PG 212 LAS. 164Shayan JuttAinda não há avaliações
- Disorders of Parathyroid GlandsDocumento52 páginasDisorders of Parathyroid GlandsDr. Akash GuptaAinda não há avaliações
- Ift PPT-1Documento21 páginasIft PPT-1Swetha Purushothaman100% (1)
- Achilles TendonDocumento30 páginasAchilles TendonMeldianaAinda não há avaliações
- Scapular Stabilization ExercisesDocumento2 páginasScapular Stabilization ExercisesnimitrisAinda não há avaliações
- Wound Healing: Santos, Patrick John S., MD First Year Resident Department of Surgery Manila MedDocumento60 páginasWound Healing: Santos, Patrick John S., MD First Year Resident Department of Surgery Manila MedJhessie ChingAinda não há avaliações
- Refrat Soft Tissue Injury MusculoskeletalDocumento38 páginasRefrat Soft Tissue Injury MusculoskeletalLina WijayaAinda não há avaliações
- General Principles of Laparoscopic Abdominal Surgery Pp2003Documento18 páginasGeneral Principles of Laparoscopic Abdominal Surgery Pp2003jategaonkarpaAinda não há avaliações
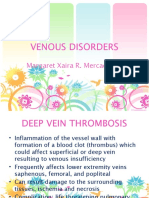
- DVT & Varicose VeinsDocumento30 páginasDVT & Varicose VeinsMargaret Xaira Rubio MercadoAinda não há avaliações
- Day Case Surgery 1LDocumento21 páginasDay Case Surgery 1LdrhiwaomerAinda não há avaliações
- FES (Functional Electrical Stimulation)Documento38 páginasFES (Functional Electrical Stimulation)Nivetha RavikumarAinda não há avaliações
- Tumescent TAPP Laparoscopic Inguinal Hernia RepairDocumento6 páginasTumescent TAPP Laparoscopic Inguinal Hernia RepairUmer KhanAinda não há avaliações
- Surgical Treatment of The "Buried" PenisDocumento6 páginasSurgical Treatment of The "Buried" PenisTengku TciAinda não há avaliações
- Suture Material and SuturingDocumento63 páginasSuture Material and SuturinganggAinda não há avaliações
- Chemical CarcinogenesisDocumento28 páginasChemical CarcinogenesisChama TlauAinda não há avaliações
- Zones of Hand: Rose Mary AntonyDocumento36 páginasZones of Hand: Rose Mary AntonyFatra FasyaAinda não há avaliações
- TractionDocumento39 páginasTractionLu IsAinda não há avaliações
- Testicular Cancer Fact Sheet PDFDocumento2 páginasTesticular Cancer Fact Sheet PDFRandaAinda não há avaliações
- Sutures عبد الرحمن الزميليDocumento54 páginasSutures عبد الرحمن الزميليعبد الرحمن خالد الزميليAinda não há avaliações
- Advanced SuturingDocumento18 páginasAdvanced SuturingAriyanie NurtaniaAinda não há avaliações
- LiverDocumento27 páginasLiverAndi Arwan AgusnawanAinda não há avaliações
- Kursus Komprehensif Bls 12-13 NOVEMBER 2013Documento19 páginasKursus Komprehensif Bls 12-13 NOVEMBER 2013Juen LohAinda não há avaliações
- Lasers in SurgeryDocumento22 páginasLasers in Surgerynuclearbrain11Ainda não há avaliações
- AppendicitisDocumento3 páginasAppendicitisPrince Jhessie L. AbellaAinda não há avaliações
- Sutures and NeedlesDocumento4 páginasSutures and Needlesjgcriste100% (4)
- Suturing and Suture MaterialsDocumento19 páginasSuturing and Suture MaterialsSangeeta BSRAinda não há avaliações
- SUTURINGDocumento6 páginasSUTURINGSahin mollickAinda não há avaliações
- Suturing: Presented By: Prof - Vijayreddy Vandali Dept of Medical-Surgical Nursing IndiaDocumento20 páginasSuturing: Presented By: Prof - Vijayreddy Vandali Dept of Medical-Surgical Nursing IndiaNamulondo Mwajib BogereAinda não há avaliações
- Suturing Materials and TechniquesDocumento29 páginasSuturing Materials and Techniquesharshini100% (1)
- Suture and NeedlesDocumento5 páginasSuture and NeedlesMabesAinda não há avaliações
- Reduction, Relocation and Splinting in Emergency Room (RASER)No EverandReduction, Relocation and Splinting in Emergency Room (RASER)Ainda não há avaliações
- What Is Coronary Heart DiseaseDocumento2 páginasWhat Is Coronary Heart DiseasePrince Jhessie L. AbellaAinda não há avaliações
- Date Time Topic Facilitator: Research Writeshop ScheduleDocumento1 páginaDate Time Topic Facilitator: Research Writeshop SchedulePrince Jhessie L. AbellaAinda não há avaliações
- Asthma: Signs That Your Asthma Is Probably Worsening IncludeDocumento7 páginasAsthma: Signs That Your Asthma Is Probably Worsening IncludePrince Jhessie L. AbellaAinda não há avaliações
- Acute Cholecystitis: What Are The Symptoms?Documento3 páginasAcute Cholecystitis: What Are The Symptoms?Prince Jhessie L. AbellaAinda não há avaliações
- AppendicitisDocumento3 páginasAppendicitisPrince Jhessie L. AbellaAinda não há avaliações
- Medication SafetyDocumento68 páginasMedication SafetyPrince Jhessie L. Abella100% (9)
- Annual Appraisal 2019 EDocumento2 páginasAnnual Appraisal 2019 EPrince Jhessie L. AbellaAinda não há avaliações
- Star Award Evaluation FormDocumento1 páginaStar Award Evaluation FormPrince Jhessie L. AbellaAinda não há avaliações
- Care of Comatose and Vulnerable PatientsDocumento32 páginasCare of Comatose and Vulnerable PatientsPrince Jhessie L. AbellaAinda não há avaliações
- CBAHI PresentationDocumento23 páginasCBAHI PresentationPrince Jhessie L. AbellaAinda não há avaliações
- Conscience FormationDocumento94 páginasConscience FormationPrince Jhessie L. AbellaAinda não há avaliações
- The Nursing Management PROCESS: An Overview: Prof. Jhessie L. Abella, RN, RM, MANDocumento30 páginasThe Nursing Management PROCESS: An Overview: Prof. Jhessie L. Abella, RN, RM, MANPrince Jhessie L. AbellaAinda não há avaliações
- CBAHI PresentationDocumento12 páginasCBAHI PresentationPrince Jhessie L. AbellaAinda não há avaliações
- Leader in MeDocumento39 páginasLeader in MePrince Jhessie L. AbellaAinda não há avaliações
- Sense of Self Efficacy Discernment of CELTECH College InstrucorsDocumento17 páginasSense of Self Efficacy Discernment of CELTECH College InstrucorsPrince Jhessie L. AbellaAinda não há avaliações
- Canadian Triage and Acuity Scale PediaDocumento30 páginasCanadian Triage and Acuity Scale PediaPrince Jhessie L. AbellaAinda não há avaliações
- Palliative Care NursingDocumento64 páginasPalliative Care NursingPrince Jhessie L. Abella100% (1)
- Diagnostic Imaging TechniquesDocumento55 páginasDiagnostic Imaging TechniquesPrince Jhessie L. AbellaAinda não há avaliações
- Nursing Curriculum DevelopmentDocumento50 páginasNursing Curriculum DevelopmentPrince Jhessie L. Abella100% (2)
- Chain of InfectionDocumento15 páginasChain of InfectionPrince Jhessie L. Abella0% (1)
- Chronic Wound Managment HMIDocumento37 páginasChronic Wound Managment HMIannisa edwarAinda não há avaliações
- Araneta Vs CA FullDocumento6 páginasAraneta Vs CA FullMia CatanAinda não há avaliações
- People V AlmazanDocumento5 páginasPeople V AlmazanGol LumAinda não há avaliações
- Vainieri 2020Documento7 páginasVainieri 2020Ayyub AlzahemAinda não há avaliações
- Actisorb Silver 220: Product ProfileDocumento12 páginasActisorb Silver 220: Product ProfileBeaulah HunidzariraAinda não há avaliações
- Old Canalicular Laceration Repair A Retrospective Study ofDocumento6 páginasOld Canalicular Laceration Repair A Retrospective Study ofMuh Syarifullah AAinda não há avaliações
- Risk For Injury Nursing Care Plan Assessment Nursing Diagnosis Planning Nursing Interventions Rationale Evaluation Subjective Data: Short Term: Goal Met Short TermDocumento3 páginasRisk For Injury Nursing Care Plan Assessment Nursing Diagnosis Planning Nursing Interventions Rationale Evaluation Subjective Data: Short Term: Goal Met Short TermSherry Ann FayeAinda não há avaliações
- Health and Safety Solutions Accident Investigation FormDocumento2 páginasHealth and Safety Solutions Accident Investigation Formhussein aliAinda não há avaliações
- NCPDocumento6 páginasNCPgenevieve kryzleiAinda não há avaliações
- PERILITE and HOT SITZDocumento3 páginasPERILITE and HOT SITZMikha BorcesAinda não há avaliações
- SEARO Proposal For Demonstration Project On R&D For Diabetes MellitusDocumento17 páginasSEARO Proposal For Demonstration Project On R&D For Diabetes Mellitussubramanyam62Ainda não há avaliações
- Matary Special Surgery 2013 (WWW - Afriqa Sat - Com)Documento419 páginasMatary Special Surgery 2013 (WWW - Afriqa Sat - Com)Ahmed Attia100% (1)
- AutopsyDocumento24 páginasAutopsyRoberto Giorgio N. Pacheco100% (1)
- Nursing Practice 2-5Documento47 páginasNursing Practice 2-5Emir Mukhtar Malcampo KamidAinda não há avaliações
- 7417 Skin Tag RemovalDocumento4 páginas7417 Skin Tag RemovalNikolaus TalloAinda não há avaliações
- Intelligence Is Like A River: The Deeper It Is, The Less Noise It Makes.Documento88 páginasIntelligence Is Like A River: The Deeper It Is, The Less Noise It Makes.reccelle_pre295747Ainda não há avaliações
- Traditional Negative Pressure Wound TherapyDocumento6 páginasTraditional Negative Pressure Wound TherapyIJAR JOURNALAinda não há avaliações
- GURPS 4e - Combat Maneuvers Cheat Sheet 1.95 by Onkl PDFDocumento2 páginasGURPS 4e - Combat Maneuvers Cheat Sheet 1.95 by Onkl PDFGlen HansardAinda não há avaliações
- People v. Encomienda G.R. No. L-26750Documento8 páginasPeople v. Encomienda G.R. No. L-26750fgAinda não há avaliações
- Discharge PlanDocumento1 páginaDischarge PlanGail GenturalezAinda não há avaliações
- Wound DebridementDocumento21 páginasWound DebridementNawal FarooqAinda não há avaliações
- Treating Dogs With MAGGOT Infestations KITDocumento3 páginasTreating Dogs With MAGGOT Infestations KITPadmavothi BharadwajAinda não há avaliações
- JurnalDocumento4 páginasJurnalIan ErvanAinda não há avaliações
- P v. Diocado GR 170567Documento11 páginasP v. Diocado GR 170567JanMarkMontedeRamosWongAinda não há avaliações
- Tokyo NOVA - Faction & Skill ListDocumento71 páginasTokyo NOVA - Faction & Skill Listluyten 789-6Ainda não há avaliações
- NCPDocumento18 páginasNCPChristian Karl B. LlanesAinda não há avaliações
- Antibiotic Prophylaxis in Surgery: Module MenuDocumento5 páginasAntibiotic Prophylaxis in Surgery: Module MenuKhairul MustafaAinda não há avaliações
- Accidents Fact SheetDocumento1 páginaAccidents Fact SheetmajikAinda não há avaliações
- First Aid Cdrrmo 2019Documento373 páginasFirst Aid Cdrrmo 2019fenan sollanoAinda não há avaliações
- V. Nursing Care Plan 1 PriorityDocumento3 páginasV. Nursing Care Plan 1 PriorityElisa Kerr100% (1)