Você também pode gostar
- Case Report Pediatric Von&JepDocumento23 páginasCase Report Pediatric Von&JepFarizan NurmushoffaAinda não há avaliações
- A Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsNo EverandA Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsAinda não há avaliações
- Aplastic AnemiaDocumento13 páginasAplastic AnemiaHazel Eñga Tiam WatAinda não há avaliações
- Hematological Alterations: Aplastic AnemiaDocumento23 páginasHematological Alterations: Aplastic Anemiajhommmmm100% (2)
- Rabies: Ragina AguilaDocumento55 páginasRabies: Ragina AguilaCharles Lester AdalimAinda não há avaliações
- Iron Deficiency AnemiaDocumento5 páginasIron Deficiency AnemiaLoiegy PaetAinda não há avaliações
- Hemolytic AnemiaDocumento9 páginasHemolytic AnemiaTheeya QuigaoAinda não há avaliações
- Hepatic EncephalopathyDocumento3 páginasHepatic EncephalopathyAnonymous GIGXKjfLAinda não há avaliações
- Pernicious AnemiaDocumento36 páginasPernicious Anemiaopesh3Ainda não há avaliações
- Glucose-6-Phosphate Dehydrogenase Deficiency - Overview: Symptom Treatment Prevention All InformationDocumento2 páginasGlucose-6-Phosphate Dehydrogenase Deficiency - Overview: Symptom Treatment Prevention All InformationJinky TenezaAinda não há avaliações
- Beta Thalassemia PathoDocumento1 páginaBeta Thalassemia PathoAngie LamoAinda não há avaliações
- Stroke and Cerebrovascular DiseaseDocumento14 páginasStroke and Cerebrovascular DiseaseMarwan M.Ainda não há avaliações
- PurpuraDocumento7 páginasPurpuraMarie Joe AbainzaAinda não há avaliações
- Megaloblastic Anemia: Red Cell DisordersDocumento17 páginasMegaloblastic Anemia: Red Cell DisordersKrishnakant Prajapati100% (1)
- Liver CirrhosisDocumento60 páginasLiver CirrhosisCamilla Zharine P. BantaAinda não há avaliações
- OsteomalaciaDocumento8 páginasOsteomalaciaRudhira KatragaddaAinda não há avaliações
- Practice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearDocumento44 páginasPractice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearSundarAinda não há avaliações
- Acute Myeloid Leukemia (Drug Study)Documento3 páginasAcute Myeloid Leukemia (Drug Study)Krisianne Mae Lorenzo FranciscoAinda não há avaliações
- Acute Lymphocytic LeukemiaDocumento12 páginasAcute Lymphocytic Leukemiajustin_saneAinda não há avaliações
- Pernicious AnemiaDocumento24 páginasPernicious AnemiaArthadian De PeraltaAinda não há avaliações
- DkaDocumento29 páginasDkaShadowSpectre0Ainda não há avaliações
- Acute Renal Failure Powerpoint PresentationDocumento18 páginasAcute Renal Failure Powerpoint PresentationSteven Paul DaclesAinda não há avaliações
- Acute Myocardial InfarctionDocumento20 páginasAcute Myocardial InfarctionDavid Christian CalmaAinda não há avaliações
- Osteogenesis ImperfectaDocumento27 páginasOsteogenesis Imperfectacode212Ainda não há avaliações
- Endometrial HyperplasiaDocumento9 páginasEndometrial HyperplasiaMelissa Aina Mohd YusofAinda não há avaliações
- Leukemia)Documento66 páginasLeukemia)Arianne BugnaAinda não há avaliações
- Ebola Virus DiseaseDocumento19 páginasEbola Virus DiseaseAuliani Annisa FebriAinda não há avaliações
- Anemia of Chronic Disease - Inflammation - UpToDateDocumento36 páginasAnemia of Chronic Disease - Inflammation - UpToDateDomenica MurilloAinda não há avaliações
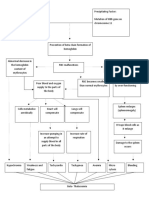
- Mechanism of HypertensionDocumento4 páginasMechanism of HypertensionAlya Putri KhairaniAinda não há avaliações
- Drug StudyDocumento5 páginasDrug StudyJanine Erika Julom BrillantesAinda não há avaliações
- Schistosomiasis Case StudyDocumento5 páginasSchistosomiasis Case Studyapi-318749549Ainda não há avaliações
- Anatomy and Phsyiology of MeningococcemiaDocumento2 páginasAnatomy and Phsyiology of MeningococcemiaKevin Comahig100% (1)
- HemophiliaDocumento60 páginasHemophiliavibhurocksAinda não há avaliações
- Hemolytic AnemiaDocumento61 páginasHemolytic AnemiaMangayarkarasi ChandrakasanAinda não há avaliações
- Case Study PneumoniaDocumento6 páginasCase Study PneumoniaBrian CornelAinda não há avaliações
- Hyperphosphatemia and HypophosphatemiaDocumento15 páginasHyperphosphatemia and HypophosphatemiaHari Prasad KAinda não há avaliações
- Acute Renal FailureDocumento25 páginasAcute Renal FailureRyan Akhmad Adhi SaputraAinda não há avaliações
- DR Amanullah Lail: Assistant Professor Paediatrics Duhs/Dmc/ChkDocumento36 páginasDR Amanullah Lail: Assistant Professor Paediatrics Duhs/Dmc/ChkpaqardAinda não há avaliações
- Pathophysiology of DiarrheaDocumento3 páginasPathophysiology of DiarrheaFathur RahmatAinda não há avaliações
- Pyloric StenosisDocumento5 páginasPyloric Stenosisensoooooooooo100% (1)
- Rafols, Janna Mae L. 3F-2C OR QuestionsDocumento8 páginasRafols, Janna Mae L. 3F-2C OR QuestionsJan Crizza Dale R. FrancoAinda não há avaliações
- Normal Values of CBCDocumento1 páginaNormal Values of CBCCherr NollAinda não há avaliações
- Sickle-Cell Anaemia EssayDocumento4 páginasSickle-Cell Anaemia Essayapi-299807117Ainda não há avaliações
- Buerger DiseaseDocumento3 páginasBuerger DiseaseElmer DizonAinda não há avaliações
- G6PD DeficiencyDocumento16 páginasG6PD DeficiencyRona SalandoAinda não há avaliações
- Case Study - Incomplete Abortion Related To APSDocumento8 páginasCase Study - Incomplete Abortion Related To APSRomeo ReyesAinda não há avaliações
- Endometriosis PresentationDocumento58 páginasEndometriosis PresentationBRI KUAinda não há avaliações
- Pernicious Anemia (B12 Deficiency)Documento38 páginasPernicious Anemia (B12 Deficiency)estieglitz1Ainda não há avaliações
- Wilms TumorDocumento12 páginasWilms TumorKath CamachoAinda não há avaliações
- Hereditary SpherocytosisDocumento16 páginasHereditary Spherocytosisrizi2008Ainda não há avaliações
- 1-Drugs Affecting Uterine Muscle ContractilityDocumento40 páginas1-Drugs Affecting Uterine Muscle ContractilityjojolilimomoAinda não há avaliações
- Pathophysiology of Nephrotic SyndromeDocumento10 páginasPathophysiology of Nephrotic Syndromejoyshe111Ainda não há avaliações
- Pediatric Nephrotic Nephritic SyndromesDocumento18 páginasPediatric Nephrotic Nephritic SyndromesBryan AtasAinda não há avaliações
- Pernicious AnemiaDocumento7 páginasPernicious AnemiaTracy PearlAinda não há avaliações
- Idiopathic Thrombocytopenic Purpura: Overview With Report of A CaseDocumento4 páginasIdiopathic Thrombocytopenic Purpura: Overview With Report of A CaseHernan GonzalezAinda não há avaliações
- Idiopathic Thrombocytopenic PurpuraDocumento2 páginasIdiopathic Thrombocytopenic PurpuraMitch Hellgirl AlmonteAinda não há avaliações
- Aplastic Anemia and Approach To Diagnosis in A Case of AnemiaDocumento19 páginasAplastic Anemia and Approach To Diagnosis in A Case of Anemia2006suzainAinda não há avaliações
- Erythrocyte Life Cycle: PathophysiologyDocumento15 páginasErythrocyte Life Cycle: PathophysiologyYeniAinda não há avaliações
- Anemia Penyakit KronisDocumento16 páginasAnemia Penyakit KronismayawjyAinda não há avaliações
- Blood Culture Manual MT - SinaiDocumento41 páginasBlood Culture Manual MT - SinaiAvi Verma100% (1)
- AnthraxDocumento12 páginasAnthraxAvi Verma100% (1)
- Iron Deficiency AnemiaDocumento1 páginaIron Deficiency AnemiaFrancis Lloyd NeriAinda não há avaliações
- Urine Culture Manual MT - SINAI PDFDocumento15 páginasUrine Culture Manual MT - SINAI PDFAvi VermaAinda não há avaliações
- B. AnthracisDocumento1 páginaB. AnthracisAvi VermaAinda não há avaliações
- NOTESDocumento1 páginaNOTESAvi VermaAinda não há avaliações
- L E CellDocumento59 páginasL E CellAvi VermaAinda não há avaliações
- ColorimeterDocumento7 páginasColorimeterAvi VermaAinda não há avaliações
- Microbio Lec 5 - StaphylococcusDocumento6 páginasMicrobio Lec 5 - Staphylococcusapi-3743217100% (2)
- Compatibility Testing For Blood TransfusionDocumento51 páginasCompatibility Testing For Blood TransfusiontaecyzAinda não há avaliações
- ImmunohistochemistryDocumento29 páginasImmunohistochemistryAvi VermaAinda não há avaliações
- Tubular Function TestDocumento12 páginasTubular Function TestAvi Verma100% (1)
- Tuberculosis: Presenter - Poonam BSC MLT 3 Year. Moderator-Dr - Neelam KaisthaDocumento39 páginasTuberculosis: Presenter - Poonam BSC MLT 3 Year. Moderator-Dr - Neelam KaisthaAvi VermaAinda não há avaliações
- Mycetoma.: Distribution: Aetiological AgentsDocumento12 páginasMycetoma.: Distribution: Aetiological AgentsAvi VermaAinda não há avaliações
- Plasma Hemoglobin and Urine Hemoglobin EstimationDocumento12 páginasPlasma Hemoglobin and Urine Hemoglobin EstimationAvi VermaAinda não há avaliações
- Liver Function TestDocumento20 páginasLiver Function TestAvi VermaAinda não há avaliações
- Respiratory Tract InfectionDocumento50 páginasRespiratory Tract InfectionAvi Verma100% (2)
- Urinary Tract Infection: Presented by - Reeta Sharma Moderator-Dr. ....Documento23 páginasUrinary Tract Infection: Presented by - Reeta Sharma Moderator-Dr. ....Avi VermaAinda não há avaliações
- Tuberculosis: Presenter - Poonam BSC MLT 3 Year. Moderator-Dr - Neelam KaisthaDocumento39 páginasTuberculosis: Presenter - Poonam BSC MLT 3 Year. Moderator-Dr - Neelam KaisthaAvi VermaAinda não há avaliações
- Lab Control of Anticagulant & TherapyDocumento33 páginasLab Control of Anticagulant & TherapyAvi VermaAinda não há avaliações
- Glomerular Function TestsDocumento26 páginasGlomerular Function TestsAvi Verma100% (1)
- Introduction of CalculiDocumento25 páginasIntroduction of CalculiAvi VermaAinda não há avaliações
- Hypersensitivity: Presenter:Prateema Gill Moderater: Dr. Niti SinghalDocumento25 páginasHypersensitivity: Presenter:Prateema Gill Moderater: Dr. Niti SinghalAvi VermaAinda não há avaliações
- RNADocumento25 páginasRNAAvi VermaAinda não há avaliações
- Gastric AnalysisDocumento23 páginasGastric AnalysisAvi VermaAinda não há avaliações
- FCE Test SampleDocumento5 páginasFCE Test SamplelennihollanderAinda não há avaliações
- Cladogram Analysis Lab Key 2015-CfDocumento3 páginasCladogram Analysis Lab Key 2015-CfRey Christine CarzonAinda não há avaliações
- Bio Circulatory System WorksheetsDocumento21 páginasBio Circulatory System WorksheetsCraft City0% (1)
- TT2 Tests EOY BDocumento4 páginasTT2 Tests EOY BJezabel MascioAinda não há avaliações
- The Laws Detailed in The Book of LeviticusDocumento14 páginasThe Laws Detailed in The Book of Leviticusdanceswithwinkles100% (3)
- Urinary System-1Documento48 páginasUrinary System-1Muhammad SajjadAinda não há avaliações
- DAoC AchievementsDocumento13 páginasDAoC AchievementsJoey FieldsAinda não há avaliações
- Feasts For The GodsDocumento79 páginasFeasts For The GodsVasile Sturzu100% (6)
- Logic Games For Young Learners 1 KeyDocumento4 páginasLogic Games For Young Learners 1 KeyKarla AndreaAinda não há avaliações
- 34 English Spelling TodayDocumento13 páginas34 English Spelling TodayabdulmusaverAinda não há avaliações
- Overlord - Volume 04 - The Lizardmen Heroes (Yen Press) (Ko) (Kitzoku) PDFDocumento332 páginasOverlord - Volume 04 - The Lizardmen Heroes (Yen Press) (Ko) (Kitzoku) PDFAmanuealAinda não há avaliações
- Cells and TissuesDocumento14 páginasCells and TissuesLawrence NemirAinda não há avaliações
- Reading Record For Oxford Reading Tree and TreetopsDocumento42 páginasReading Record For Oxford Reading Tree and TreetopsM Atif Ali GorayaAinda não há avaliações
- IndomethacinDocumento17 páginasIndomethacinRajpal Singh KochharAinda não há avaliações
- Blok 22 - Skenario D - 2019 Neonatal Case: ST TH THDocumento6 páginasBlok 22 - Skenario D - 2019 Neonatal Case: ST TH THNur akilaAinda não há avaliações
- Dengue JournalDocumento4 páginasDengue JournalRohitKumarAinda não há avaliações
- Animal StoriesDocumento13 páginasAnimal StoriesNora AfidaAinda não há avaliações
- Tajweed Rules of The Qur'anDocumento25 páginasTajweed Rules of The Qur'anridwanmdAinda não há avaliações
- Lepra ReactionDocumento24 páginasLepra ReactionSWAPAN KUMAR SARKAR100% (2)
- Society of Primitive Technology - Earth Skills, Wilderness Survival (PDFDrive)Documento156 páginasSociety of Primitive Technology - Earth Skills, Wilderness Survival (PDFDrive)Eng. Alexandre AlbinoAinda não há avaliações
- Case PresentationDocumento11 páginasCase PresentationJOhn DiCeAinda não há avaliações
- Harry - Jimenz - Letter of Invitation PDFDocumento1 páginaHarry - Jimenz - Letter of Invitation PDFSampath Ravula100% (1)
- Earth and Life Sciences SLHTQ2 3Documento9 páginasEarth and Life Sciences SLHTQ2 3Melissa GerzonAinda não há avaliações
- 1 SMDocumento10 páginas1 SMNurul Hikmah Haetapi AminAinda não há avaliações
- Shadows of Esteren The Tri-Kazelian Bestiary PDFDocumento29 páginasShadows of Esteren The Tri-Kazelian Bestiary PDFAnonymous iL4zr96LKB100% (2)
- Ao 2011-0002Documento7 páginasAo 2011-0002Suzette Paredes-RagosAinda não há avaliações
- Survival KitDocumento8 páginasSurvival KitedGarKazy77Ainda não há avaliações
- Tropical Oceans: Word SearchDocumento2 páginasTropical Oceans: Word SearchAgrobacterium TumefaciensAinda não há avaliações
- 1.1 The Little School BusDocumento156 páginas1.1 The Little School BusAifa Afeeqa JamilanAinda não há avaliações