Você também pode gostar
- Electrocardiographs, Multichannel Interpretive: Scope of This Product ComparisonDocumento83 páginasElectrocardiographs, Multichannel Interpretive: Scope of This Product ComparisonchanlalAinda não há avaliações
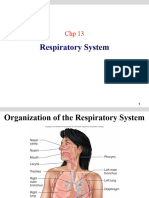
- Respiratory PhysiologyDocumento98 páginasRespiratory PhysiologySurya SuryaAinda não há avaliações
- Chapter 22Documento12 páginasChapter 22Jenn ParksAinda não há avaliações
- Respiration - VentilationDocumento102 páginasRespiration - VentilationSodeinde SimeonAinda não há avaliações
- Anatomi Fisiologi Pernapasan Dr. MDocumento87 páginasAnatomi Fisiologi Pernapasan Dr. MARIF BSAinda não há avaliações
- Respiratory System: Departement of Physiology Medical Faculty of Universitas Sumatera UtaraDocumento142 páginasRespiratory System: Departement of Physiology Medical Faculty of Universitas Sumatera Utara292Vien HardiyantiAinda não há avaliações
- Chapter 12Documento28 páginasChapter 12براءة أحمد السلاماتAinda não há avaliações
- Chapter 12Documento28 páginasChapter 12Ammar SmadiAinda não há avaliações
- M132 Respiratory 2022Documento28 páginasM132 Respiratory 2022Bana ItanAinda não há avaliações
- Respiratory PhysiologyDocumento30 páginasRespiratory PhysiologyBarbara Sakura RiawanAinda não há avaliações
- Compliance of LungsDocumento37 páginasCompliance of LungsJasir KhanAinda não há avaliações
- Ventilation Dead Space Ventilation Physiology of RespirationDocumento55 páginasVentilation Dead Space Ventilation Physiology of RespirationkuhutansittinurhalizaAinda não há avaliações
- L - 1 Physiology of Respiration IDocumento25 páginasL - 1 Physiology of Respiration Ikaukab azimAinda não há avaliações
- L - 1 Physiology of Respiration IDocumento28 páginasL - 1 Physiology of Respiration IshahabsworldAinda não há avaliações
- Ani̇mal Respiratory System PhysiologyDocumento18 páginasAni̇mal Respiratory System PhysiologyNajafova SuadaAinda não há avaliações
- Lecture 1.6 Mechanics of Breathing II - Dr. AlkhateebDocumento37 páginasLecture 1.6 Mechanics of Breathing II - Dr. AlkhateebJohn KashAinda não há avaliações
- Lecture Notes On Respiratory Physiology PDFDocumento33 páginasLecture Notes On Respiratory Physiology PDFMiles HuiAinda não há avaliações
- University of Guyana School of Medicine Med 1106 - Physiology I DR Kalima ThompsonDocumento66 páginasUniversity of Guyana School of Medicine Med 1106 - Physiology I DR Kalima ThompsonKAinda não há avaliações
- 12.respiratory SystemDocumento52 páginas12.respiratory SystemRulani PrinceAinda não há avaliações
- Respiratory PhysiologyDocumento68 páginasRespiratory PhysiologyDjAinda não há avaliações
- Biofluid Mechanics Chapter 3Documento35 páginasBiofluid Mechanics Chapter 3AbcdAinda não há avaliações
- Anatomi Fisiologi PernapasanDocumento87 páginasAnatomi Fisiologi PernapasanAndre ChundawanAinda não há avaliações
- Respiratoryfunctionandimportancetoanesthesia Final 140103050711 Phpapp02Documento62 páginasRespiratoryfunctionandimportancetoanesthesia Final 140103050711 Phpapp02rijjorajooAinda não há avaliações
- Dyamics of Respiration Composition VentilationDocumento30 páginasDyamics of Respiration Composition VentilationUsama SajidAinda não há avaliações
- Respiratory Physiology: By: DR Muhammad Arslan Qureshi FCPS AnesthesiaDocumento59 páginasRespiratory Physiology: By: DR Muhammad Arslan Qureshi FCPS AnesthesiaSarmadAinda não há avaliações
- Exchange of Gases Between The Atmosphere & The LungsDocumento21 páginasExchange of Gases Between The Atmosphere & The LungsJulee Pearl GangosoAinda não há avaliações
- Respiratory System: M.AzhariDocumento142 páginasRespiratory System: M.AzhariLili ManaoAinda não há avaliações
- 1.anatomy & Physiology of AirwayDocumento54 páginas1.anatomy & Physiology of Airwayqwerty hrAinda não há avaliações
- Explaination To Answers of Respiration Test Date: 16.08.2020Documento1 páginaExplaination To Answers of Respiration Test Date: 16.08.2020Shubham SsAinda não há avaliações
- Respiratory Physiology NoteDocumento19 páginasRespiratory Physiology NotePeter Wong0% (1)
- Respiratory System-1Documento84 páginasRespiratory System-1pranjal raiAinda não há avaliações
- The Mechanics of Breathing: Mashmum Shababa ShahidDocumento31 páginasThe Mechanics of Breathing: Mashmum Shababa ShahidSHANJIDA ALI RIAAinda não há avaliações
- Respiratory SystemDocumento32 páginasRespiratory SystemvhieeelgbmAinda não há avaliações
- Compliance of Lung 2003Documento13 páginasCompliance of Lung 2003Narendra Bhattarai100% (1)
- Respiratory System: Dr. Agung Kurniawan, MkesDocumento31 páginasRespiratory System: Dr. Agung Kurniawan, MkesJojo BodhoAinda não há avaliações
- AND Lung Ventilation: VolumesDocumento27 páginasAND Lung Ventilation: VolumesShaina OturdoAinda não há avaliações
- Dr. Sunita Saxena - Breathing and Exchange of GassesDocumento48 páginasDr. Sunita Saxena - Breathing and Exchange of GassesDivya AgarawalAinda não há avaliações
- Pulmonary Mumbo Jumbo - MartinezDocumento12 páginasPulmonary Mumbo Jumbo - MartinezMartinez_DOAinda não há avaliações
- Airflow: Group 4 - Respiratory System VentilationDocumento18 páginasAirflow: Group 4 - Respiratory System VentilationNathalieCaracaAinda não há avaliações
- OLM. Physiology - Lung ComplianceDocumento39 páginasOLM. Physiology - Lung Compliancedagehi6880Ainda não há avaliações
- Mechanics of Breathing.Documento39 páginasMechanics of Breathing.Eba DadoughAinda não há avaliações
- Fundamentalof Ventilation & PacemakerDocumento22 páginasFundamentalof Ventilation & PacemakerLucila Lugo100% (1)
- Anatomi Dan Fisiologi RespirasiDocumento22 páginasAnatomi Dan Fisiologi RespirasinortonaingAinda não há avaliações
- Ventilasi ParuDocumento59 páginasVentilasi ParuDwi Rizky LestariAinda não há avaliações
- Ventilation and Respiratory VolumesDocumento10 páginasVentilation and Respiratory Volumesalthea jade villadongaAinda não há avaliações
- 1.airway, Airflow, Ventilation and DiffusionDocumento64 páginas1.airway, Airflow, Ventilation and DiffusionEbin EbenezerAinda não há avaliações
- Respiratory System Uploaded On Dow PortalDocumento52 páginasRespiratory System Uploaded On Dow PortalAyesha MasoodAinda não há avaliações
- Johnson Jerry Alan Chinese Medical Qigong Therapy Vol 5-141-160Documento20 páginasJohnson Jerry Alan Chinese Medical Qigong Therapy Vol 5-141-160toanbauAinda não há avaliações
- Introduction To Respiratory System-2020Documento27 páginasIntroduction To Respiratory System-2020Izlan AidilAinda não há avaliações
- M. Hill Physiology (22) Mechanics of BreathingDocumento32 páginasM. Hill Physiology (22) Mechanics of BreathingEfrain AnayaAinda não há avaliações
- Respiration: Physiology / 2009-10 Dr. Ahmad .S. AlarabiDocumento23 páginasRespiration: Physiology / 2009-10 Dr. Ahmad .S. AlarabiJerome EkohAinda não há avaliações
- Respiratory Physiology IIDocumento83 páginasRespiratory Physiology IIDeea LobonțiuAinda não há avaliações
- Respiratory SystemDocumento23 páginasRespiratory SystembettyAinda não há avaliações
- 3-4 Respiratory V&CDocumento55 páginas3-4 Respiratory V&CCumar TimirAinda não há avaliações
- TARIQUL - ISLAM - GOLDARMechanism of Respiration.2021-04-30mechanism of RespirationDocumento10 páginasTARIQUL - ISLAM - GOLDARMechanism of Respiration.2021-04-30mechanism of RespirationJuwairiyya AliyuAinda não há avaliações
- Respiratory Notes and SlideDocumento33 páginasRespiratory Notes and SlideChristina Gonez100% (1)
- Bio 215 Topic 7 RespiratoryDocumento46 páginasBio 215 Topic 7 RespiratoryYara BeainiAinda não há avaliações
- Atelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesNo EverandAtelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesAinda não há avaliações
- Pulmonary Function Tests in Clinical PracticeNo EverandPulmonary Function Tests in Clinical PracticeAli AltalagNota: 5 de 5 estrelas5/5 (1)
- Xducers & P-MonitorsDocumento22 páginasXducers & P-MonitorschanlalAinda não há avaliações
- 8-ECG Fni$Documento61 páginas8-ECG Fni$chanlalAinda não há avaliações
- NKC 0104Documento9 páginasNKC 0104chanlalAinda não há avaliações
- Technical Seminar: Electrocardiograph (ECG) Ecg-K Ecg- K・ECG- KDocumento60 páginasTechnical Seminar: Electrocardiograph (ECG) Ecg-K Ecg- K・ECG- Kchanlal0% (1)
- Nehon ECGDocumento4 páginasNehon ECGchanlalAinda não há avaliações
- Nehon ECG - PDF 2Documento2 páginasNehon ECG - PDF 2chanlalAinda não há avaliações
- Outlines of Mechanical VentilationDocumento21 páginasOutlines of Mechanical VentilationchanlalAinda não há avaliações
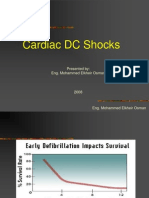
- Cardiac DC Shocks: Presented By: Eng. Mohammed Elkheir OsmanDocumento18 páginasCardiac DC Shocks: Presented By: Eng. Mohammed Elkheir OsmanchanlalAinda não há avaliações
- 3-EEG Fni$Documento50 páginas3-EEG Fni$chanlalAinda não há avaliações
- ECG TestDocumento3 páginasECG TestchanlalAinda não há avaliações
- Electro SurgeryDocumento19 páginasElectro SurgerychanlalAinda não há avaliações
- Nehon ECGDocumento4 páginasNehon ECGchanlalAinda não há avaliações
- NKC 0104Documento9 páginasNKC 0104chanlalAinda não há avaliações
- Ventricular Fibrillation Contraction Heart Muscles.: Is A Serious Cardiac Emergency Resulting From Asynchronous of TheDocumento28 páginasVentricular Fibrillation Contraction Heart Muscles.: Is A Serious Cardiac Emergency Resulting From Asynchronous of ThechanlalAinda não há avaliações
- Tec5500 Om eDocumento334 páginasTec5500 Om echanlal100% (1)
- Basic Principle, Operation and Maintenance: Aqeel Ahmed KhanDocumento18 páginasBasic Principle, Operation and Maintenance: Aqeel Ahmed KhanchanlalAinda não há avaliações
- ECG TestDocumento3 páginasECG TestchanlalAinda não há avaliações
- High Frequency Heat TherapyDocumento56 páginasHigh Frequency Heat TherapychanlalAinda não há avaliações
- TEC5500 Tech Seminar 2008Documento35 páginasTEC5500 Tech Seminar 2008chanlalAinda não há avaliações
- New HV Capacitor 5500 - 7600 - 7700Documento1 páginaNew HV Capacitor 5500 - 7600 - 7700chanlalAinda não há avaliações
- TEC5500 OM p10 - 9 Battery Test PDFDocumento3 páginasTEC5500 OM p10 - 9 Battery Test PDFchanlalAinda não há avaliações
- TEC5500 Error CodeDocumento7 páginasTEC5500 Error CodechanlalAinda não há avaliações
- Defibrillation - Basic 55 For DistributorDocumento14 páginasDefibrillation - Basic 55 For DistributorchanlalAinda não há avaliações
- Cardiology - Defibrillator: A: Silence Alarm E: Setup ModeDocumento4 páginasCardiology - Defibrillator: A: Silence Alarm E: Setup ModechanlalAinda não há avaliações
- HV Relay Unit CheckDocumento1 páginaHV Relay Unit CheckchanlalAinda não há avaliações
- Biphasic DefbrillationDocumento16 páginasBiphasic DefbrillationchanlalAinda não há avaliações
- Ventilator System CoursDocumento1 páginaVentilator System CourschanlalAinda não há avaliações
- Review SlidesDocumento8 páginasReview SlideschanlalAinda não há avaliações
- Behaviour of Investors in Indian Equity Markets: Submitted byDocumento26 páginasBehaviour of Investors in Indian Equity Markets: Submitted byDibyanshu AmanAinda não há avaliações
- Malefactor ClassDocumento23 páginasMalefactor ClassMatthew Duncan100% (6)
- Muller-Lyer IllusionDocumento3 páginasMuller-Lyer Illusionsara VermaAinda não há avaliações
- The Role of Personalization, Engagement and Trust in Online CommunitiesDocumento17 páginasThe Role of Personalization, Engagement and Trust in Online CommunitiesAbiAinda não há avaliações
- Biometric Security ConcernsDocumento27 páginasBiometric Security ConcernsprinceuchenduAinda não há avaliações
- Radiopharmaceutical Production: History of Cyclotrons The Early Years at BerkeleyDocumento31 páginasRadiopharmaceutical Production: History of Cyclotrons The Early Years at BerkeleyNguyễnKhươngDuyAinda não há avaliações
- Interfaces and Inheritance in JavaDocumento1 páginaInterfaces and Inheritance in JavaegdejuanaAinda não há avaliações
- Asset Management PlanDocumento160 páginasAsset Management Planbkalatus1100% (1)
- Olinger v. The Church of Jesus Christ of Latter Day Saints Et Al - Document No. 1Documento4 páginasOlinger v. The Church of Jesus Christ of Latter Day Saints Et Al - Document No. 1Justia.comAinda não há avaliações
- Nurse-Patient Trust RelationshipDocumento12 páginasNurse-Patient Trust RelationshipMarina Costa100% (1)
- Oration For Jon Kyle ValdehuezaDocumento2 páginasOration For Jon Kyle ValdehuezaJakes ValAinda não há avaliações
- Rediscovering The True Self Through TheDocumento20 páginasRediscovering The True Self Through TheManuel Ortiz100% (1)
- Role of Courts in Granting Bails and Bail Reforms: TH THDocumento1 páginaRole of Courts in Granting Bails and Bail Reforms: TH THSamarth VikramAinda não há avaliações
- Ministry of Truth Big Brother Watch 290123Documento106 páginasMinistry of Truth Big Brother Watch 290123Valentin ChirilaAinda não há avaliações
- Filipino HousesDocumento4 páginasFilipino HousesjackAinda não há avaliações
- Resume of Masterchef Contestant, Melissa GutierrezDocumento3 páginasResume of Masterchef Contestant, Melissa GutierrezMikhail GalatinovAinda não há avaliações
- Roman Villas at Tor Marancia and CentocelleDocumento10 páginasRoman Villas at Tor Marancia and CentocelleIgor ĆirkovićAinda não há avaliações
- Quarter 2-Module 7 Social and Political Stratification: Department of Education Republic of The PhilippinesDocumento21 páginasQuarter 2-Module 7 Social and Political Stratification: Department of Education Republic of The Philippinestricia100% (5)
- Match The Animal With Its NameDocumento4 páginasMatch The Animal With Its Namekawa kawka kawuniaAinda não há avaliações
- Defending A Dogma: Between Grice, Strawson and Quine: Elvis ImafidonDocumento10 páginasDefending A Dogma: Between Grice, Strawson and Quine: Elvis ImafidonYang Wen-LiAinda não há avaliações
- Arsu and AzizoDocumento123 páginasArsu and AzizoZebu BlackAinda não há avaliações
- Lecture 6Documento7 páginasLecture 6Shuja MirAinda não há avaliações
- A100K10873 VSP-12-Way Technical ManualDocumento20 páginasA100K10873 VSP-12-Way Technical Manualchufta50% (2)
- Number SystemsDocumento165 páginasNumber SystemsapamanAinda não há avaliações
- Arif Dirlik - The Origins of Chinese Communism-Oxford University Press, USA (1989)Documento335 páginasArif Dirlik - The Origins of Chinese Communism-Oxford University Press, USA (1989)Denisa FeisalAinda não há avaliações
- Managing Ambiguity and ChangeDocumento7 páginasManaging Ambiguity and ChangeTracey FeboAinda não há avaliações
- Dopamine What It Is, Function & SymptomsDocumento7 páginasDopamine What It Is, Function & SymptomsRaj KumarAinda não há avaliações
- Class 12 Accountancy HHDocumento58 páginasClass 12 Accountancy HHkomal barotAinda não há avaliações
- Institute of Actuaries of India: Subject CT3-Probability and Mathematical Statistics May 2008 ExaminationDocumento10 páginasInstitute of Actuaries of India: Subject CT3-Probability and Mathematical Statistics May 2008 ExaminationeuticusAinda não há avaliações
- Baltimore Catechism No. 2 (Of 4)Documento64 páginasBaltimore Catechism No. 2 (Of 4)gogelAinda não há avaliações