Você também pode gostar
- Diabetes Type 2 Treatment AlgorithmDocumento26 páginasDiabetes Type 2 Treatment AlgorithmLokesh KhuranaAinda não há avaliações
- Terapi Oran Dan InsulinDocumento35 páginasTerapi Oran Dan InsulinAnonymous spBVX6t30UAinda não há avaliações
- Diabetes Management UpdateDocumento64 páginasDiabetes Management UpdatethisarAinda não há avaliações
- Managent DMT2 KabDocumento49 páginasManagent DMT2 KabNoorvita SRAinda não há avaliações
- Management of DMDocumento9 páginasManagement of DMnurul izzatiAinda não há avaliações
- DM Medical Nutritional TherapyDocumento5 páginasDM Medical Nutritional TherapyNeil AlviarAinda não há avaliações
- Obesity in Adults - Drug Therapy - UpToDate PDFDocumento59 páginasObesity in Adults - Drug Therapy - UpToDate PDFDiana TovarAinda não há avaliações
- Diabetes MelitusDocumento57 páginasDiabetes MelitusArzyad Analis KesehatanAinda não há avaliações
- Management of Diabetes MellitusDocumento4 páginasManagement of Diabetes MellitusshasadharaAinda não há avaliações
- Bpjs Case Study DiabetesDocumento33 páginasBpjs Case Study DiabetesAdhi TjahyadiAinda não há avaliações
- JDM20120200002 37731682Documento5 páginasJDM20120200002 37731682Raissa Andi SoekrisnoAinda não há avaliações
- Diabetes Melitus IIDocumento8 páginasDiabetes Melitus IIharunnuranAinda não há avaliações
- Clinical Nutrition Guidelina For Overwight and Obese Adults With DiabetesDocumento10 páginasClinical Nutrition Guidelina For Overwight and Obese Adults With Diabetesjose luis VallejoAinda não há avaliações
- Treatment MedscapeDocumento3 páginasTreatment MedscapeEvi BaeAinda não há avaliações
- 3 Lifestyle Management: SIGN 116: Management of DiabetesDocumento12 páginas3 Lifestyle Management: SIGN 116: Management of DiabetesMohamed SalamAinda não há avaliações
- Meal Planning For DiabetesDocumento29 páginasMeal Planning For DiabetesnurulahdiahAinda não há avaliações
- 2nd Case Session ToT CPG HPTDocumento127 páginas2nd Case Session ToT CPG HPThakimahsAinda não há avaliações
- Type 2 Diabetes MellitusDocumento4 páginasType 2 Diabetes MellitusMazhar WarisAinda não há avaliações
- Cad Guidelines Secondary 10.04Documento2 páginasCad Guidelines Secondary 10.04Wira LinAinda não há avaliações
- Management of Persistent Hyperglycemia in Type 2 Diabetes MellitusDocumento47 páginasManagement of Persistent Hyperglycemia in Type 2 Diabetes MellitusEslam khedrAinda não há avaliações
- Nfs 774 Case StudyDocumento37 páginasNfs 774 Case Studyapi-533845626Ainda não há avaliações
- 6 Intro To DMDocumento38 páginas6 Intro To DMSPUB HPONTIANAinda não há avaliações
- Five Steps in Management of DMDocumento62 páginasFive Steps in Management of DMarti tyagitaAinda não há avaliações
- Treatment Protocol For Type-II Diabetes MellitusDocumento7 páginasTreatment Protocol For Type-II Diabetes MellitusSOUMIK MANDALAinda não há avaliações
- DM Ppt. NewDocumento26 páginasDM Ppt. NewRio Ramon HilarioAinda não há avaliações
- Working Your Way Through Adas t2d Treatment AlgorithmDocumento61 páginasWorking Your Way Through Adas t2d Treatment AlgorithmNgọc BíchAinda não há avaliações
- Obesity ManagementDocumento24 páginasObesity ManagementAshutosh Singh100% (1)
- Joslin Center Sobrepeso y ObesidadDocumento7 páginasJoslin Center Sobrepeso y ObesidadSilvia Lozano MayorAinda não há avaliações
- Diabetes 1Documento13 páginasDiabetes 1n_catalinAinda não há avaliações
- Diabetes: Amjad Al ShdaifatDocumento94 páginasDiabetes: Amjad Al ShdaifatRand AhmadAinda não há avaliações
- Insulin in DMDocumento46 páginasInsulin in DMask1400Ainda não há avaliações
- Interim Assignment 2Documento2 páginasInterim Assignment 2NiteshAinda não há avaliações
- Oral Diabetic MedicationDocumento26 páginasOral Diabetic MedicationTaimoor BaigAinda não há avaliações
- Diabetes ManagementDocumento9 páginasDiabetes ManagementdhearawrsAinda não há avaliações
- Diabetes Melitus Dan KomplikasinyaDocumento60 páginasDiabetes Melitus Dan Komplikasinyahandiwijaya_85Ainda não há avaliações
- ADA Standards of Care For Diabetes 2013Documento4 páginasADA Standards of Care For Diabetes 2013Syawal PratamaAinda não há avaliações
- Non-Insulin Therapies for Type 2 DiabetesDocumento40 páginasNon-Insulin Therapies for Type 2 DiabetesscribdAinda não há avaliações
- Indonesia's Growing Diabetes EpidemicDocumento28 páginasIndonesia's Growing Diabetes EpidemicAdhi TjahyadiAinda não há avaliações
- Final 4Documento11 páginasFinal 4api-722911357Ainda não há avaliações
- Effect of Diet On Type 2 Diabetes Mellitus: A Review.: Sami, W Ansari, T Butt, N.S Hamid, M.R. 2017Documento5 páginasEffect of Diet On Type 2 Diabetes Mellitus: A Review.: Sami, W Ansari, T Butt, N.S Hamid, M.R. 2017Yayang SavitaAinda não há avaliações
- Sitagliptin vs Glipizide Efficacy and Safety in T2DM PatientsDocumento29 páginasSitagliptin vs Glipizide Efficacy and Safety in T2DM PatientslordizzatAinda não há avaliações
- Self Monitoring of Blood GlucoseDocumento12 páginasSelf Monitoring of Blood GlucoseJay R PlogioAinda não há avaliações
- Initial Management of Blood Glucose in Adults With Type 2 Diabetes MellitusDocumento22 páginasInitial Management of Blood Glucose in Adults With Type 2 Diabetes MellitusSaleh M.Ainda não há avaliações
- Jurnal Pilihan PDFDocumento4 páginasJurnal Pilihan PDFIWayanSuparthanayaAinda não há avaliações
- Diabetes PDFDocumento4 páginasDiabetes PDFAadit GuptaAinda não há avaliações
- Diabetes Trends Bilog DelaCruz Rodriguez TubungbanuaDocumento15 páginasDiabetes Trends Bilog DelaCruz Rodriguez TubungbanuaJoshua Hilapo TubungbanuaAinda não há avaliações
- Efficacy of Semaglutide in A Subcutaneous and An Oral FormulationDocumento11 páginasEfficacy of Semaglutide in A Subcutaneous and An Oral FormulationNewtonRibeiroAinda não há avaliações
- Diabetes GuidelinesDocumento3 páginasDiabetes GuidelinesHossam_Fayed_4294Ainda não há avaliações
- Diabetes Melitus & Sindroma Metabolik PITDocumento48 páginasDiabetes Melitus & Sindroma Metabolik PITharryruswantoAinda não há avaliações
- Presentation Indonesia Sep 8 2022Documento88 páginasPresentation Indonesia Sep 8 2022yuni chanAinda não há avaliações
- Diabetes Type 2 PharmacotherapyDocumento37 páginasDiabetes Type 2 Pharmacotherapyali khanAinda não há avaliações
- Eyip PRP PresentationDocumento32 páginasEyip PRP Presentationapi-265314029Ainda não há avaliações
- Nutritional Considerations in Type 2 Diabetes MellitusDocumento39 páginasNutritional Considerations in Type 2 Diabetes MellitusNhiAinda não há avaliações
- Choosing The Best Oral Diabetic Agents in t2 Diabetes Mellitusphysicians Challenge 2155 6156 1000797Documento7 páginasChoosing The Best Oral Diabetic Agents in t2 Diabetes Mellitusphysicians Challenge 2155 6156 1000797silvanaAinda não há avaliações
- Diabetes MellitusDocumento24 páginasDiabetes Mellitus2f6ys4x9tgAinda não há avaliações
- 04 DiabetesDocumento10 páginas04 DiabetesMary Marjorie RodaviaAinda não há avaliações
- Nutrition in DMDocumento33 páginasNutrition in DMkero R.habibAinda não há avaliações
- The Control of The Glucose Triad - ChallengesDocumento26 páginasThe Control of The Glucose Triad - ChallengesIoana ZahaAinda não há avaliações
- Canadian: Hypoglycemia: Understanding The EnemyDocumento8 páginasCanadian: Hypoglycemia: Understanding The EnemyndistantiAinda não há avaliações
- Asma AkutDocumento31 páginasAsma AkutFathin Rahmani SalmanAinda não há avaliações
- Aspect Neurology: Tetanus, Rabies, Malaria, TBC Thypoid, HivDocumento108 páginasAspect Neurology: Tetanus, Rabies, Malaria, TBC Thypoid, HivFathin Rahmani SalmanAinda não há avaliações
- 2.facial PainDocumento31 páginas2.facial PainFathin Rahmani SalmanAinda não há avaliações
- Refreshing AppDocumento31 páginasRefreshing AppFathin Rahmani SalmanAinda não há avaliações
- Infectious Diseases: PSPD FKK Umj Anwar Wardy WDocumento48 páginasInfectious Diseases: PSPD FKK Umj Anwar Wardy WFathin Rahmani SalmanAinda não há avaliações
- 316013Documento8 páginas316013Fathin Rahmani SalmanAinda não há avaliações
- The Development of Road Transport Safety in IndonesiaDocumento24 páginasThe Development of Road Transport Safety in IndonesiaFathin Rahmani SalmanAinda não há avaliações
- 3 PainDocumento24 páginas3 PainFathin Rahmani SalmanAinda não há avaliações
- Photo TheraphyDocumento7 páginasPhoto TheraphyFathin Rahmani SalmanAinda não há avaliações
- Serum Transaminase Levels and Dengue Shock Syndrome in ChildrenDocumento5 páginasSerum Transaminase Levels and Dengue Shock Syndrome in ChildrenNofanny FeliciaAinda não há avaliações
- Health Informatic FK UmjDocumento24 páginasHealth Informatic FK UmjFathin Rahmani SalmanAinda não há avaliações
- Serum Transaminase Levels and Dengue Shock Syndrome in ChildrenDocumento5 páginasSerum Transaminase Levels and Dengue Shock Syndrome in ChildrenNofanny FeliciaAinda não há avaliações
- Bioethics - Medical Law - Human Right: Muhammadiyah University of JakartaDocumento56 páginasBioethics - Medical Law - Human Right: Muhammadiyah University of JakartaFathin Rahmani SalmanAinda não há avaliações
- Etika Penelitian DR - MeitaDocumento32 páginasEtika Penelitian DR - MeitaFathin Rahmani SalmanAinda não há avaliações
- Industrial Noise and Its Effects On HumansDocumento6 páginasIndustrial Noise and Its Effects On HumansFathin Rahmani SalmanAinda não há avaliações
- Della Sala Memory MCI PatientsDocumento17 páginasDella Sala Memory MCI PatientsSri AsmawatiAinda não há avaliações
- Diabetes Mellitus Drug ChartDocumento3 páginasDiabetes Mellitus Drug Chartlui.stephanie1751100% (1)
- Pemberian Insulin KMBDocumento36 páginasPemberian Insulin KMBerdhian jatiAinda não há avaliações
- Diabetes - FDA-Approved Diabetes MedicinesDocumento3 páginasDiabetes - FDA-Approved Diabetes MedicinesArunAinda não há avaliações
- Types of Insulin According to Mode of ActionDocumento1 páginaTypes of Insulin According to Mode of ActionAssem Ashraf Khidhr100% (1)
- New Microsoft Word DocumentDocumento2 páginasNew Microsoft Word Documenteslambasuony98Ainda não há avaliações
- Review Jurnal Farmakologi GiziDocumento7 páginasReview Jurnal Farmakologi Giziade100% (1)
- Tableau Antidiabetiques 2018 enDocumento1 páginaTableau Antidiabetiques 2018 enpraefatioAinda não há avaliações
- Cara Penyimpanan ObatDocumento2 páginasCara Penyimpanan ObatLhian NieezAinda não há avaliações
- Diabetes PDFDocumento5 páginasDiabetes PDFErica MailigAinda não há avaliações
- PR 00073 (Dpho) JuniDocumento3 páginasPR 00073 (Dpho) JuniTitha RahmiAinda não há avaliações
- Insulin Chart 05032012 PDFDocumento1 páginaInsulin Chart 05032012 PDFTiffany CrittendenAinda não há avaliações
- Continuous Subcutaneous Insulin InfusionDocumento6 páginasContinuous Subcutaneous Insulin Infusiondonny elhamdouniAinda não há avaliações
- Choosing The Best Oral Diabetic Agents in t2 Diabetes Mellitusphysicians Challenge 2155 6156 1000797Documento7 páginasChoosing The Best Oral Diabetic Agents in t2 Diabetes Mellitusphysicians Challenge 2155 6156 1000797silvanaAinda não há avaliações
- Simplifying Insulin Therapy With Ryzodeg: DR Mohammad Irfan SPPDDocumento37 páginasSimplifying Insulin Therapy With Ryzodeg: DR Mohammad Irfan SPPDmohammad.irfanAinda não há avaliações
- Insulin Options in Type 2 Diabetes Following Market Discontinuation of Mixtard 30Documento5 páginasInsulin Options in Type 2 Diabetes Following Market Discontinuation of Mixtard 30Chetan KhaitanAinda não há avaliações
- Premix Analogue VS. Premix Human Insulin Clinical DifferencesDocumento36 páginasPremix Analogue VS. Premix Human Insulin Clinical Differencesborn_321118403Ainda não há avaliações
- Diabetes Management & Insulin InitiationDocumento39 páginasDiabetes Management & Insulin InitiationTaufiqurrochman Nur AminAinda não há avaliações
- Insulin Initiation GuidanceDocumento4 páginasInsulin Initiation GuidanceRahma WatiAinda não há avaliações
- Lista Gratuidade EAN 14.02.2020Documento10 páginasLista Gratuidade EAN 14.02.2020Lidia Dias GonçalvesAinda não há avaliações
- Medicamentele prescrisse pentru tratamentul afecțiunilor persoanelor prevăzute în Legea nr. 95/2006Documento19 páginasMedicamentele prescrisse pentru tratamentul afecțiunilor persoanelor prevăzute în Legea nr. 95/2006amocatoAinda não há avaliações
- Nyicil Borang Poli Penyakit DalamDocumento3 páginasNyicil Borang Poli Penyakit Dalamrachma rfiAinda não há avaliações
- Diabetes Mellitus: Apt. Lelly Winduhani M.Farm - KlinDocumento30 páginasDiabetes Mellitus: Apt. Lelly Winduhani M.Farm - KlinListiaAinda não há avaliações
- Farmakologi DMDocumento41 páginasFarmakologi DMZainul MuttaqinAinda não há avaliações
- Product Presentation EZELIN 2019 PDFDocumento29 páginasProduct Presentation EZELIN 2019 PDFratnaAinda não há avaliações
- Anti DiabeticDocumento34 páginasAnti DiabeticEJ GabaoAinda não há avaliações
- Insulin Analogs ELISA Kits Offered by KRISHGEN BIOSYSTEMS.Documento2 páginasInsulin Analogs ELISA Kits Offered by KRISHGEN BIOSYSTEMS.KRISHGEN BIOSYSTEMSAinda não há avaliações
- Pengobatan Diabetes Mellitus Type 2Documento28 páginasPengobatan Diabetes Mellitus Type 2mursidstone.mursidAinda não há avaliações
- Panduan Praktik Klinis Ugd PopoolivDocumento49 páginasPanduan Praktik Klinis Ugd PopoolivrusliAinda não há avaliações
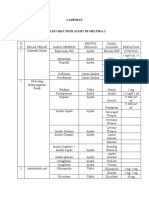
- RS Melinda 2 Lampiran Daftar Obat High Alert dan LASADocumento6 páginasRS Melinda 2 Lampiran Daftar Obat High Alert dan LASARestika Eria PutriAinda não há avaliações
- 7 OAD DR - Elly 2015Documento52 páginas7 OAD DR - Elly 2015ainAinda não há avaliações