Você também pode gostar
- Acute Coronary SyndromeDocumento57 páginasAcute Coronary SyndromePreety ShresthaAinda não há avaliações
- Cardio DiseasesDocumento77 páginasCardio Diseasesrea bentayaoAinda não há avaliações
- Konsep Tatalaksana Pada ImaDocumento57 páginasKonsep Tatalaksana Pada Imariska silviaAinda não há avaliações
- Pericardial DiseaseDocumento50 páginasPericardial DiseasengrhoAinda não há avaliações
- How To Detect and To Treat EarlierDocumento59 páginasHow To Detect and To Treat EarlierFaisal ShaldyAinda não há avaliações
- Acute Coronary Syndrome Sindroma Koroner AkutDocumento50 páginasAcute Coronary Syndrome Sindroma Koroner AkutWinda Ayu PurnamasariAinda não há avaliações
- Acute Coronary Syndrome Sindroma Koroner Akut: PUJI RAHAYU,.S.Kep.,Ners, M.KepDocumento52 páginasAcute Coronary Syndrome Sindroma Koroner Akut: PUJI RAHAYU,.S.Kep.,Ners, M.KepLabu SiamAinda não há avaliações
- Acute Coronary Syndromes-PresentationDocumento86 páginasAcute Coronary Syndromes-Presentationpatange jayaprakash rahul100% (4)
- Ischemic Stroke: Deb Roberts, M.D., Ph.D. Washington University School of MedicineDocumento129 páginasIschemic Stroke: Deb Roberts, M.D., Ph.D. Washington University School of MedicinegiftyAinda não há avaliações
- Coronary Arterial Disease: S Chapter 60 1657Documento26 páginasCoronary Arterial Disease: S Chapter 60 1657Staen KisAinda não há avaliações
- Ischemic Heart Disease: Dr. Pearl Myers Path Fall 2011 With Acknowledgement To DR SADocumento67 páginasIschemic Heart Disease: Dr. Pearl Myers Path Fall 2011 With Acknowledgement To DR SADylan KremerAinda não há avaliações
- Acute Coronary Syndrome Sindroma Koroner Akut: Toni Mustahsani Aprami, DR., SPPD, SPJPDocumento57 páginasAcute Coronary Syndrome Sindroma Koroner Akut: Toni Mustahsani Aprami, DR., SPPD, SPJPrian susantoAinda não há avaliações
- ACS LectureDocumento74 páginasACS Lecturekarin amalia sabrinaAinda não há avaliações
- Acute Coronary Syndrome Sindroma Koroner AkutDocumento57 páginasAcute Coronary Syndrome Sindroma Koroner Akutendah100% (1)
- ACS LectureDocumento76 páginasACS Lecture21701101047 Laksmita AnggaraniAinda não há avaliações
- Microvascular Angina (MVA) : Carlos Ernesto Cabrera VelascoDocumento32 páginasMicrovascular Angina (MVA) : Carlos Ernesto Cabrera VelascoAndres Andrade ErasoAinda não há avaliações
- Cardiac Biomarker 2014Documento52 páginasCardiac Biomarker 2014karin amalia sabrina100% (1)
- Askep Pada Acute Coronary Syndrome AcsDocumento62 páginasAskep Pada Acute Coronary Syndrome Acsdefi rhAinda não há avaliações
- Penyakit Kardiovaskular Yang Sering DijumpaiDocumento121 páginasPenyakit Kardiovaskular Yang Sering Dijumpaiandikaagus13Ainda não há avaliações
- Cardiogenic Shock and Pulmonary EdemaDocumento41 páginasCardiogenic Shock and Pulmonary EdemaChristian Gallardo, MD100% (7)
- MCQ 2019 Part 1 UseDocumento94 páginasMCQ 2019 Part 1 UseWanny WattakavanichAinda não há avaliações
- Acute Coronary Syndrome Update: Charles Shoalmire, MSN, RN, ACNP-BCDocumento31 páginasAcute Coronary Syndrome Update: Charles Shoalmire, MSN, RN, ACNP-BCDwi Akbarina YahyaAinda não há avaliações
- Myocardial InfarctionDocumento40 páginasMyocardial InfarctionHIRANGER100% (3)
- Approach To Acute Coronary SyndromeDocumento25 páginasApproach To Acute Coronary Syndromeزكريا الحسناتAinda não há avaliações
- Pathophysiology/Epidemiology of Acute Coronary Syndromes: 1 2 November 2019Documento15 páginasPathophysiology/Epidemiology of Acute Coronary Syndromes: 1 2 November 2019anasAinda não há avaliações
- MCQ 2019 Part 1 UseDocumento94 páginasMCQ 2019 Part 1 UseMimmey YeniwAinda não há avaliações
- Myocardial InfarctionDocumento43 páginasMyocardial InfarctiondeeptiAinda não há avaliações
- 4.18 Mankad Echo in Systemic DiseaseDocumento97 páginas4.18 Mankad Echo in Systemic DiseaseDiana_anca6Ainda não há avaliações
- Biochemical Cardiac Markers in Acute Coronary Syndrome: by DR L A GovenderDocumento43 páginasBiochemical Cardiac Markers in Acute Coronary Syndrome: by DR L A GovenderMichelle BandongAinda não há avaliações
- 02.emergency CardiologyDocumento135 páginas02.emergency Cardiologyapi-19916399Ainda não há avaliações
- Shock: Cardiogenic & ObstructiveDocumento31 páginasShock: Cardiogenic & Obstructive黃昱睿Ainda não há avaliações
- CARDIOMYOPATHIESDocumento80 páginasCARDIOMYOPATHIESNadun MethwadaneAinda não há avaliações
- Acute Coronary Syndrome: by Ho NisaDocumento58 páginasAcute Coronary Syndrome: by Ho NisaShre RanjithamAinda não há avaliações
- Acute Myocardial Infarction: Sarah Priore RN BSNDocumento53 páginasAcute Myocardial Infarction: Sarah Priore RN BSNAngnaKalsiAinda não há avaliações
- Anaesthetic Management of A Patient With Ischaemic Heart Disease Undergoing Non Cardiac SurgeryDocumento72 páginasAnaesthetic Management of A Patient With Ischaemic Heart Disease Undergoing Non Cardiac SurgeryDebasis SahooAinda não há avaliações
- Coronary Heart Disease 3Documento47 páginasCoronary Heart Disease 3Silvia RAinda não há avaliações
- Lecture 3 - IHDDocumento29 páginasLecture 3 - IHDقاسم اليوسفيAinda não há avaliações
- Acute Coronary Syndrome 052014Documento91 páginasAcute Coronary Syndrome 052014Fatahillah NazarAinda não há avaliações
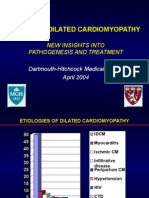
- Idiopathic Dilated Cardiomyopathy: New Insights Into Pathogenesis and TreatmentDocumento51 páginasIdiopathic Dilated Cardiomyopathy: New Insights Into Pathogenesis and TreatmentAlexandra PataAinda não há avaliações
- Stroke by Dr. AM IyagbaDocumento44 páginasStroke by Dr. AM IyagbaDr. Amb. Monday ZaccheausAinda não há avaliações
- Coronary Artery Disease and Acute Coronary Syndrome Myocardial InfarctionDocumento3 páginasCoronary Artery Disease and Acute Coronary Syndrome Myocardial InfarctionsenaringAinda não há avaliações
- Universal Definition of MIDocumento25 páginasUniversal Definition of MImikaAinda não há avaliações
- Cardiogenic Shock - FINALDocumento79 páginasCardiogenic Shock - FINALIgor StefanetAinda não há avaliações
- Curs 9 Myocarditis CardiomyopathyDocumento41 páginasCurs 9 Myocarditis CardiomyopathyIliescu DenisaAinda não há avaliações
- Step Up To MedicineDocumento68 páginasStep Up To MedicineAmadou N'Dow100% (1)
- Myocardial InfarctionDocumento34 páginasMyocardial InfarctionMeera ANN AJIAinda não há avaliações
- Myocardial Infarction: Maj Aswathy Ganesh I Year MSC (N) Con, AfmcDocumento45 páginasMyocardial Infarction: Maj Aswathy Ganesh I Year MSC (N) Con, AfmcAswathy ganeshAinda não há avaliações
- Acs SGD 8 - 20240308 - 051618 - 0000Documento13 páginasAcs SGD 8 - 20240308 - 051618 - 0000Sarah JesikaAinda não há avaliações
- Chest Pain: Differential Diagnosis Walid TARCHA, MD Umc Rizk HospitalDocumento56 páginasChest Pain: Differential Diagnosis Walid TARCHA, MD Umc Rizk HospitalAli B. SafadiAinda não há avaliações
- Myocardial InfarctionDocumento33 páginasMyocardial InfarctionArchana GaonkarAinda não há avaliações
- Myocarditis: Dr. S G Shyam Lakshman Senior Resident Dept of CardiologyDocumento62 páginasMyocarditis: Dr. S G Shyam Lakshman Senior Resident Dept of CardiologyDr.sonuAinda não há avaliações
- Acute MiDocumento61 páginasAcute MiMalueth AnguiAinda não há avaliações
- Nstemi Non ST Elevation Myocardial InfarctionDocumento45 páginasNstemi Non ST Elevation Myocardial Infarctionpeni_dwi100% (1)
- Coronary Artery DiseaseDocumento60 páginasCoronary Artery DiseaseliliAinda não há avaliações
- Pathogenesis of Cardiac DisordersDocumento28 páginasPathogenesis of Cardiac DisordersUdochukwu EnebeAinda não há avaliações
- Acute Coronary SyndromesDocumento82 páginasAcute Coronary Syndromesmidras taranAinda não há avaliações
- Drugs and Defibrillation: Department of Anesthesiology & Reanimation General Hospital TasikmalayaDocumento20 páginasDrugs and Defibrillation: Department of Anesthesiology & Reanimation General Hospital TasikmalayaAfrida Sahestina100% (1)
- Which Dial Do I Turn! The Essence of Mechanical VentilationDocumento54 páginasWhich Dial Do I Turn! The Essence of Mechanical VentilationKang Wisit TheaAinda não há avaliações
- Anesthesia For High Risk PatientDocumento5 páginasAnesthesia For High Risk PatientAfrida SahestinaAinda não há avaliações
- I II III: DNA Binding Ligand Binding Activation Domain Dimerization Nuclear Localization SilencingDocumento6 páginasI II III: DNA Binding Ligand Binding Activation Domain Dimerization Nuclear Localization SilencingAfrida SahestinaAinda não há avaliações
- Ctev (Congenital Talipes Equinus Varus)Documento9 páginasCtev (Congenital Talipes Equinus Varus)Afrida SahestinaAinda não há avaliações
- Notes On Peck&Coyle Practical CriticismDocumento10 páginasNotes On Peck&Coyle Practical CriticismLily DameAinda não há avaliações
- A Team - Group - ESG Handbook 2021 July 2021Documento69 páginasA Team - Group - ESG Handbook 2021 July 2021Prajwala JankarAinda não há avaliações
- Furuno FM 8700 Users Manual 429122Documento102 páginasFuruno FM 8700 Users Manual 429122Igor MaranguanheAinda não há avaliações
- Comparison of Ozone Vs Uv in WaterDocumento1 páginaComparison of Ozone Vs Uv in WaterRajesh PandeyAinda não há avaliações
- Asms 02 0033Documento6 páginasAsms 02 0033Delfia AkiharyAinda não há avaliações
- Disorders of The Endocrine System and Dental ManagementDocumento63 páginasDisorders of The Endocrine System and Dental ManagementSanni FatimaAinda não há avaliações
- Grade 7 Information Writing: The Bulldog: A Dog Like No OtherDocumento5 páginasGrade 7 Information Writing: The Bulldog: A Dog Like No Otherapi-202727113Ainda não há avaliações
- Board of Technical Education Uttar Pradesh Lucknow: CODE 2298Documento2 páginasBoard of Technical Education Uttar Pradesh Lucknow: CODE 2298Md Shaaz100% (1)
- VK-53 (ВК-53) Erecting Cut-Out Switch: Maintenance ManualDocumento76 páginasVK-53 (ВК-53) Erecting Cut-Out Switch: Maintenance ManualhaileAinda não há avaliações
- r315 Quick Start PDFDocumento80 páginasr315 Quick Start PDFfdsfasdsfadsAinda não há avaliações
- Head To Toe Assessment GuideDocumento2 páginasHead To Toe Assessment GuideSara SabraAinda não há avaliações
- The Girl Who CanDocumento4 páginasThe Girl Who CanMadhu50% (2)
- B11R Jonckheere JHV2 SpecDocumento1 páginaB11R Jonckheere JHV2 SpecVishwanath SeetaramAinda não há avaliações
- Wolfi Landstreicher - Willful Disobedience - Number 3Documento32 páginasWolfi Landstreicher - Willful Disobedience - Number 3populaererAinda não há avaliações
- YearbookDocumento55 páginasYearbookGODWIN IRIMORENAinda não há avaliações
- Iso 3932 1976Documento8 páginasIso 3932 1976NaveedAinda não há avaliações
- IAL Hemanta Kumar KarDocumento639 páginasIAL Hemanta Kumar KarTalita Abrani100% (4)
- Manual Placa Mae Ga 945gcmx-s2 6.6Documento72 páginasManual Placa Mae Ga 945gcmx-s2 6.6luisb3toAinda não há avaliações
- TNB Ar2011Documento334 páginasTNB Ar2011Duncan LeeAinda não há avaliações
- SpiralsDocumento12 páginasSpiralskkglobalAinda não há avaliações
- Text For Number 1-3: How To Make Passion Fruit Juice IngredientsDocumento4 páginasText For Number 1-3: How To Make Passion Fruit Juice Ingredientsakmal maulanaAinda não há avaliações
- Statistical Mechanics PDFDocumento578 páginasStatistical Mechanics PDFraymon6666100% (6)
- Hirschsprung's Disease - AthigamanDocumento128 páginasHirschsprung's Disease - Athigamanprived100% (4)
- Material Specifications: Low Carbon Steel, Hot Rolled Sheet and StripDocumento5 páginasMaterial Specifications: Low Carbon Steel, Hot Rolled Sheet and Striptim0% (1)
- Mathematics Specialist Unit 3A: VectorsDocumento4 páginasMathematics Specialist Unit 3A: VectorsMahir MahmoodAinda não há avaliações
- 365-M - City Bus Route & Timings, Bangalore (BMTC) Map, First & Last BusDocumento10 páginas365-M - City Bus Route & Timings, Bangalore (BMTC) Map, First & Last BusER Aditya DasAinda não há avaliações
- Unit-4 - Hypothesis TestingDocumento24 páginasUnit-4 - Hypothesis TestingMANTHAN JADHAVAinda não há avaliações
- Bendable ConcreteDocumento21 páginasBendable ConcreteJulia Sebastian0% (1)
- 1414-Electric Room 1 Calculation Report Rev.02Documento28 páginas1414-Electric Room 1 Calculation Report Rev.02zakariaelrayesusaAinda não há avaliações
- A Lesson About SpringDocumento7 páginasA Lesson About SpringKatjaAinda não há avaliações