Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- NCPDocumento4 páginasNCPJhuRise Ann ManganaAinda não há avaliações
- Drug Name Dosage/ Route/ Freque NCY Classifi-Cation Indication Contra - Indication Mechanism of Action Adverse Reaction Nursing ResponsibilitiesDocumento10 páginasDrug Name Dosage/ Route/ Freque NCY Classifi-Cation Indication Contra - Indication Mechanism of Action Adverse Reaction Nursing ResponsibilitiesJhuRise Ann ManganaAinda não há avaliações
- Definition/Description: Rheumatoid Arthritis Asthma Multiple SclerosisDocumento8 páginasDefinition/Description: Rheumatoid Arthritis Asthma Multiple SclerosisJhuRise Ann ManganaAinda não há avaliações
- Bone Marrow Depression - Lung Collapse & Complications - Brain Damage - Liver DamageDocumento1 páginaBone Marrow Depression - Lung Collapse & Complications - Brain Damage - Liver DamageJhuRise Ann ManganaAinda não há avaliações
- Buerger's DiseaseDocumento4 páginasBuerger's DiseaseJhuRise Ann ManganaAinda não há avaliações
- Taxation II-Cases and DigestsDocumento33 páginasTaxation II-Cases and DigestsJhuRise Ann ManganaAinda não há avaliações
- Risk FactorsDocumento1 páginaRisk FactorsJhuRise Ann ManganaAinda não há avaliações
- Acute Gastroenteritis: Escherichia ColiDocumento2 páginasAcute Gastroenteritis: Escherichia ColiJhuRise Ann ManganaAinda não há avaliações
- Letter of IntentDocumento18 páginasLetter of IntentJhuRise Ann ManganaAinda não há avaliações
- DefibrillatorDocumento14 páginasDefibrillatorJhuRise Ann ManganaAinda não há avaliações
- Anus, Rectum, and Prostate AssessmentDocumento7 páginasAnus, Rectum, and Prostate AssessmentJhuRise Ann ManganaAinda não há avaliações
- Ugib NCPDocumento5 páginasUgib NCPJhuRise Ann Mangana100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Body Alchemy: The Shredded AcademyDocumento6 páginasBody Alchemy: The Shredded AcademyMATHEWS MATHEWSAinda não há avaliações
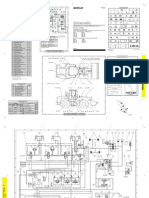
- Cat02 HeadDocumento8 páginasCat02 HeadpaolaAinda não há avaliações
- Emirates A380 PDFDocumento1 páginaEmirates A380 PDFNur TangkianAinda não há avaliações
- 2D 20160629Documento4 páginas2D 20160629anorith88Ainda não há avaliações
- List of SongDocumento4 páginasList of SongKrzysztof GieAinda não há avaliações
- FHO DischargeDocumento1 páginaFHO DischargeVarghese NellimoottilAinda não há avaliações
- Mercedes Benz CLA 2019 PDFDocumento16 páginasMercedes Benz CLA 2019 PDFMiAinda não há avaliações
- Recreation and Sport Management Template 1 1Documento2 páginasRecreation and Sport Management Template 1 1api-689066520Ainda não há avaliações
- Queen Songs: Name: - DateDocumento1 páginaQueen Songs: Name: - DateAnonymous K3WNW5ZopAinda não há avaliações
- Physical Education Practical Schedule 2019 20 PDFDocumento8 páginasPhysical Education Practical Schedule 2019 20 PDFDivyapratap Singh RathoreAinda não há avaliações
- Bearing Designation Numbers, SuffexDocumento12 páginasBearing Designation Numbers, SuffexWajahat Ali KhanAinda não há avaliações
- Straight-A Student Weekly Schedule by Daniel WongDocumento1 páginaStraight-A Student Weekly Schedule by Daniel WongSapphire Anwai100% (2)
- 10th July, 2011Documento4 páginas10th July, 2011ZnRosePocAinda não há avaliações
- Types of EventsDocumento6 páginasTypes of EventsBernalyn ManaogAinda não há avaliações
- Mini Six Character SheetDocumento1 páginaMini Six Character SheetJoaquin AlonsoAinda não há avaliações
- Orla Us Letter Paper PDFDocumento25 páginasOrla Us Letter Paper PDFAsif K100% (2)
- 1 Unit DynamicsDocumento4 páginas1 Unit DynamicsmanojAinda não há avaliações
- Jordan Fitness CatDocumento144 páginasJordan Fitness CatAndrew Richard ThompsonAinda não há avaliações
- D&D Character Sheet 18Documento3 páginasD&D Character Sheet 18greta ubermenschAinda não há avaliações
- A5 Operation ManualDocumento10 páginasA5 Operation ManualAlexandr Ivanov Sarmiento100% (1)
- Manual 950GDocumento4 páginasManual 950Gabumagico85% (13)
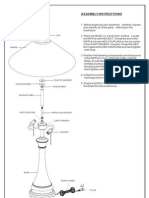
- Assembly Instructions: FinialDocumento1 páginaAssembly Instructions: Finialdayshift5Ainda não há avaliações
- Headcount Senarai Murid 2011Documento34 páginasHeadcount Senarai Murid 2011Rafidah Che SaadAinda não há avaliações
- #9 #9 Memphis Depay Depay: Sub MenuDocumento1 página#9 #9 Memphis Depay Depay: Sub MenuMohammad AlzeerAinda não há avaliações
- D&D 3e - Tiles - Battlemaps - Dungeon Rooms Vol VIDocumento27 páginasD&D 3e - Tiles - Battlemaps - Dungeon Rooms Vol VIRuppert Smooker Jr.100% (1)
- 'Ve Lost My Purse. Have You Ever Seen A Snake?: 1 2 Present Perfect Simple (1) Ever, NeverDocumento2 páginas'Ve Lost My Purse. Have You Ever Seen A Snake?: 1 2 Present Perfect Simple (1) Ever, NeverNatalia Maria Gallo AlvarezAinda não há avaliações
- Nemesis Rules Summary V4Documento6 páginasNemesis Rules Summary V4Xan CamposAinda não há avaliações
- Zsa LitaDocumento150 páginasZsa LitaSam Valdez0% (1)
- BUỔI 5.1 - KEYDocumento23 páginasBUỔI 5.1 - KEYQuynh Vu AnhAinda não há avaliações
- Mansions of Madness Second Editon Rules ReferenceDocumento24 páginasMansions of Madness Second Editon Rules ReferenceGeorge AlexandrisAinda não há avaliações