Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- TNPSC Sample Paper 3 PDFDocumento40 páginasTNPSC Sample Paper 3 PDFShiva Shankar PandianAinda não há avaliações
- Gmpplus Ba7 en 20180901 PDFDocumento29 páginasGmpplus Ba7 en 20180901 PDFdanuAinda não há avaliações
- PPG Reviewer For ShsDocumento5 páginasPPG Reviewer For ShsGoldwin RamirezAinda não há avaliações
- The Yearling: Study GuideDocumento13 páginasThe Yearling: Study GuideDaniel PalermoAinda não há avaliações
- Ihn General Training Reading Practice Test 6 Section 1 Questions 1 - 13Documento14 páginasIhn General Training Reading Practice Test 6 Section 1 Questions 1 - 13Anonymous f5qGAcZYAinda não há avaliações
- Shadows of Esteren The Tri-Kazelian Bestiary PDFDocumento29 páginasShadows of Esteren The Tri-Kazelian Bestiary PDFAnonymous iL4zr96LKB100% (2)
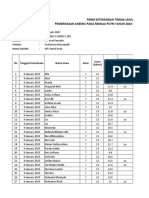
- Pemeriksaan Anemia SMP Darul MaarifDocumento38 páginasPemeriksaan Anemia SMP Darul MaarifPuskesmas BanyuputihAinda não há avaliações
- Dental Examination Record FormDocumento2 páginasDental Examination Record FormNurse AnnAinda não há avaliações
- Musical Instruments of AfricaDocumento3 páginasMusical Instruments of AfricaSitti Nur HabingAinda não há avaliações
- Email.: by Foozi SilagiDocumento9 páginasEmail.: by Foozi SilagiHasifa KonsoAinda não há avaliações
- Branchial Arch SyndromesDocumento7 páginasBranchial Arch SyndromesVita Dental PachucaAinda não há avaliações
- FeygodsDocumento6 páginasFeygodsZhori DuberryAinda não há avaliações
- Piaget's Stages of Cognitive DevelopmentDocumento15 páginasPiaget's Stages of Cognitive DevelopmentCristy Quirong SorialAinda não há avaliações
- Winsor McCayDocumento8 páginasWinsor McCayNat UrwinAinda não há avaliações
- Ountable Nouns: A Dog Is An AnimalDocumento9 páginasOuntable Nouns: A Dog Is An AnimalJoseMa AralAinda não há avaliações
- Book of Arcane Magic - WE - Reborn Soul Sorcerer Bloodline PDFDocumento3 páginasBook of Arcane Magic - WE - Reborn Soul Sorcerer Bloodline PDFJohn FrangosAinda não há avaliações
- Lesson 9 MorphologyDocumento51 páginasLesson 9 Morphologymarta_srg100% (2)
- Animal Welfare Act As AmendedDocumento5 páginasAnimal Welfare Act As AmendedJoel C AgraAinda não há avaliações
- 1.1 The Little School BusDocumento156 páginas1.1 The Little School BusAifa Afeeqa JamilanAinda não há avaliações
- How To Tell Wild AnimalsDocumento20 páginasHow To Tell Wild AnimalsShreyansh SahuAinda não há avaliações
- List Produk Mm99: Harga Jual Yang Disarankan NO Nama Barang HargaDocumento2 páginasList Produk Mm99: Harga Jual Yang Disarankan NO Nama Barang HargadadaotaAinda não há avaliações
- Language Stimulation NotebookDocumento60 páginasLanguage Stimulation NotebookScribdTranslationsAinda não há avaliações
- Do Animals Go To Heaven? C.S. Lewis On Animal ImmortalityDocumento3 páginasDo Animals Go To Heaven? C.S. Lewis On Animal Immortalitymushysector8049100% (1)
- Project 4ed - Level 2 - Photocopiable Activities - AudioscriptsDocumento4 páginasProject 4ed - Level 2 - Photocopiable Activities - AudioscriptsSzilvi KonczolAinda não há avaliações
- General Classification of MicrofossilsDocumento18 páginasGeneral Classification of MicrofossilsMujahid Ahmed KhanAinda não há avaliações
- Visser (2012) Report On The Phyisical Status of Morgan at Loro ParqueDocumento35 páginasVisser (2012) Report On The Phyisical Status of Morgan at Loro ParqueTim Zimmermann100% (2)
- July 2009 Go Guide Newsletter The MountaineersDocumento8 páginasJuly 2009 Go Guide Newsletter The MountaineersMountaineersAinda não há avaliações
- G1-Unit 3-Lesson 12 - Day 1: 1. Review VocabularyDocumento7 páginasG1-Unit 3-Lesson 12 - Day 1: 1. Review VocabularyarchurbaAinda não há avaliações
- Test Your Memory: Good Citizens Always Wear Stout ShoesDocumento3 páginasTest Your Memory: Good Citizens Always Wear Stout ShoesdanielaAinda não há avaliações
- LAW158 Essay 6Documento4 páginasLAW158 Essay 6darshan UrsAinda não há avaliações