Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Coding Case StudiesDocumento2 páginasCoding Case Studiesapi-385484216100% (1)
- Sacs 2.0 SlideDocumento20 páginasSacs 2.0 SlideAlfiantAinda não há avaliações
- Tension PneumothoraxDocumento23 páginasTension PneumothoraxQiqii Hatchi100% (1)
- Schoenbaum Implant Prosthetics in The Aesthetic Zone Science Protocol TechniquesDocumento24 páginasSchoenbaum Implant Prosthetics in The Aesthetic Zone Science Protocol TechniquesЮля КолмаковаAinda não há avaliações
- 75178347Documento5 páginas75178347Ana Di JayaAinda não há avaliações
- Renu GargDocumento3 páginasRenu GargAna Di JayaAinda não há avaliações
- A Pilot Evaluation of Saline Sonohysterography For Postmenopausal Bleeding With Thickened EndometriumDocumento4 páginasA Pilot Evaluation of Saline Sonohysterography For Postmenopausal Bleeding With Thickened EndometriumAna Di JayaAinda não há avaliações
- Pengobatan Pada Tiap KomplikasiDocumento6 páginasPengobatan Pada Tiap KomplikasiAna Di JayaAinda não há avaliações
- HydrotubationDocumento4 páginasHydrotubationAna Di Jaya100% (1)
- Viral Encephalitis: Etiology, Clinical Features, Diagnosis and ManagementDocumento12 páginasViral Encephalitis: Etiology, Clinical Features, Diagnosis and ManagementAna Di JayaAinda não há avaliações
- Journal of Medical Case ReportsDocumento4 páginasJournal of Medical Case ReportsAna Di JayaAinda não há avaliações
- HydrotubationDocumento4 páginasHydrotubationAna Di Jaya100% (1)
- Leiomyoma and Rhabdomyoma of The Vagina Vaginal MyomaDocumento5 páginasLeiomyoma and Rhabdomyoma of The Vagina Vaginal MyomaAna Di JayaAinda não há avaliações
- Case Report: Vaginal Myomectomy For A Thirteen-Centimeter Anterior MyomaDocumento4 páginasCase Report: Vaginal Myomectomy For A Thirteen-Centimeter Anterior MyomaAna Di JayaAinda não há avaliações
- Hypovolemic Shock Due To Massive Edema of A Pedunculated Uterine Myoma After DeliveryDocumento4 páginasHypovolemic Shock Due To Massive Edema of A Pedunculated Uterine Myoma After DeliveryAna Di JayaAinda não há avaliações
- Efficacy of Micronised Vaginal Progesterone Versus Oral Dydrogestrone in The Treatment of Irregular Dysfunctional Uterine Bleeding: A Pilot Randomised Controlled TrialDocumento5 páginasEfficacy of Micronised Vaginal Progesterone Versus Oral Dydrogestrone in The Treatment of Irregular Dysfunctional Uterine Bleeding: A Pilot Randomised Controlled TrialAna Di JayaAinda não há avaliações
- Who Guidlines Pregnancy Woman 2010 PDFDocumento117 páginasWho Guidlines Pregnancy Woman 2010 PDFAna Di JayaAinda não há avaliações
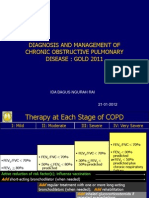
- Rountable Copd Jan 2012Documento71 páginasRountable Copd Jan 2012Ana Di JayaAinda não há avaliações
- WHO Dengue Guidelines 2013Documento160 páginasWHO Dengue Guidelines 2013Jason MirasolAinda não há avaliações
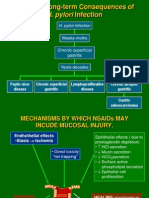
- 2 Pathogenesis TukakLambungDocumento30 páginas2 Pathogenesis TukakLambungAna Di JayaAinda não há avaliações
- Vol361and2topic04 PDFDocumento6 páginasVol361and2topic04 PDFAna Di JayaAinda não há avaliações
- Cotrimoxazole Profilaxis Hiv Who Guidlines PDFDocumento68 páginasCotrimoxazole Profilaxis Hiv Who Guidlines PDFAna Di JayaAinda não há avaliações
- Case of A Womenwith Acute Onset of Chest Pain PDFDocumento9 páginasCase of A Womenwith Acute Onset of Chest Pain PDFAna Di JayaAinda não há avaliações
- Case of Adrenal Nodule in A 59 Yrs Old Women PDFDocumento8 páginasCase of Adrenal Nodule in A 59 Yrs Old Women PDFAna Di JayaAinda não há avaliações
- Case of Adrenal Nodule in A 59 Yrs Old Women PDFDocumento8 páginasCase of Adrenal Nodule in A 59 Yrs Old Women PDFAna Di JayaAinda não há avaliações
- Case of A Woman With Cough and Lung Nodule PDFDocumento9 páginasCase of A Woman With Cough and Lung Nodule PDFAna Di JayaAinda não há avaliações
- Case of Impaired Renal Funtion PDFDocumento1 páginaCase of Impaired Renal Funtion PDFAna Di JayaAinda não há avaliações
- Case of A Woman With Obesity, DM An Hypertension PDFDocumento10 páginasCase of A Woman With Obesity, DM An Hypertension PDFAna Di JayaAinda não há avaliações
- Case of Bladder Carcinoma PDFDocumento9 páginasCase of Bladder Carcinoma PDFAna Di JayaAinda não há avaliações
- Case Report .Hepatic Failure PDFDocumento4 páginasCase Report .Hepatic Failure PDFAna Di JayaAinda não há avaliações
- Case of A Womenwith Acute Onset of Chest Pain PDFDocumento9 páginasCase of A Womenwith Acute Onset of Chest Pain PDFAna Di JayaAinda não há avaliações
- Case of Boy With Slowing Growth, Delayed Puberty PDFDocumento11 páginasCase of Boy With Slowing Growth, Delayed Puberty PDFAna Di JayaAinda não há avaliações
- Case of Bladder Carcinoma PDFDocumento9 páginasCase of Bladder Carcinoma PDFAna Di JayaAinda não há avaliações
- Activity # 3 - Research JournalDocumento3 páginasActivity # 3 - Research Journalcayla mae carlosAinda não há avaliações
- Variability and Accuracy of Sahlis Method InEstimation of Haemoglobin ConcentrationDocumento8 páginasVariability and Accuracy of Sahlis Method InEstimation of Haemoglobin Concentrationastrii 08Ainda não há avaliações
- International Classification of Function, Disabiltiy and HealthDocumento31 páginasInternational Classification of Function, Disabiltiy and Healthsri subhikshaAinda não há avaliações
- Review Cirugía Preprotésica. ArtículoDocumento9 páginasReview Cirugía Preprotésica. ArtículoAnita Estela Batz MatulAinda não há avaliações
- 199-Article Text-1111-1-10-20230613Documento7 páginas199-Article Text-1111-1-10-20230613Yayu AngrianAinda não há avaliações
- Vital Signs Procedures ChecklistDocumento3 páginasVital Signs Procedures ChecklistharpreetAinda não há avaliações
- MORPHINEDocumento39 páginasMORPHINEShlok RathodAinda não há avaliações
- Drugs requiring loading dosesDocumento1 páginaDrugs requiring loading dosesandirio7486Ainda não há avaliações
- Final Draft - Project 3Documento8 páginasFinal Draft - Project 3api-710214550Ainda não há avaliações
- Organophosphorus Insecticide Induced Hemorrhagic Pancreatitis - A Case ReportDocumento3 páginasOrganophosphorus Insecticide Induced Hemorrhagic Pancreatitis - A Case ReportIOSRjournalAinda não há avaliações
- Medical-Surgical Nursing 75 Items TestDocumento13 páginasMedical-Surgical Nursing 75 Items Testwiffato25% (4)
- Aluminium Foil For Smoking DrugsDocumento6 páginasAluminium Foil For Smoking Drugscamille64Ainda não há avaliações
- Tumor Lysis SyndromeDocumento12 páginasTumor Lysis Syndromeapi-647779956Ainda não há avaliações
- Perez TMC-213 Module-2Documento4 páginasPerez TMC-213 Module-2NISHA MIKLE MACULAinda não há avaliações
- 525 FullDocumento9 páginas525 FulldianaAinda não há avaliações
- Frequency of Hyponatraemia and Hypokalaemia in Malnourished Children With Acute DiarrhoeaDocumento4 páginasFrequency of Hyponatraemia and Hypokalaemia in Malnourished Children With Acute DiarrhoeaRaja Bajak LautAinda não há avaliações
- Effective Use of Behavioral Care PlansDocumento27 páginasEffective Use of Behavioral Care PlansZahraa Ali dawoodAinda não há avaliações
- Ec041 Medical ElectronicsDocumento2 páginasEc041 Medical ElectronicsJaya VeniAinda não há avaliações
- COVID-19 Hypercoagulability Mechanisms ReviewDocumento13 páginasCOVID-19 Hypercoagulability Mechanisms ReviewMartha OktaviaAinda não há avaliações
- Poster Ramesh MMDocumento5 páginasPoster Ramesh MMRameshKrishnanAinda não há avaliações
- Sound Finf in 280722Documento13 páginasSound Finf in 280722jongsu kimAinda não há avaliações
- Nines P Bautista, MD, MSDocumento12 páginasNines P Bautista, MD, MSadnep1991Ainda não há avaliações
- Con TovaDocumento2 páginasCon Tovasheik muhtasimAinda não há avaliações
- Chapter 8A Neonatal Emergencies.Documento35 páginasChapter 8A Neonatal Emergencies.Sai NathAinda não há avaliações
- BEmONC - Training ManualDocumento263 páginasBEmONC - Training ManualdiribaAinda não há avaliações
- Perioperative Management of The Patients With Liver DiseaseDocumento94 páginasPerioperative Management of The Patients With Liver DiseaseUmar Farooq GondalAinda não há avaliações