Você também pode gostar
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- INTERWELL Anchored Production Straddle Product SheetDocumento2 páginasINTERWELL Anchored Production Straddle Product SheetDavid Pit FermiereAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Lecture 38Documento10 páginasLecture 38Deepak GuptaAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Most Important Electrical Engineering NTS Based Short QuestionsDocumento63 páginasMost Important Electrical Engineering NTS Based Short QuestionsnageenAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- UNIT-5 International Dimensions To Industrial Relations: ObjectivesDocumento27 páginasUNIT-5 International Dimensions To Industrial Relations: ObjectivesManish DwivediAinda não há avaliações
- Major Head of AccountsDocumento9 páginasMajor Head of AccountsArun EmmiAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- NABARD Grade A 2020 Phase 2 ESI ARDDocumento6 páginasNABARD Grade A 2020 Phase 2 ESI ARDrohit bhosadAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- At4 886-12Documento110 páginasAt4 886-12scotty2hotty28100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Exp 4 Centrifugal CompressorDocumento11 páginasExp 4 Centrifugal CompressorFaris HamirAinda não há avaliações
- Effects of Various Liquid Organic Solvents On Solvent-Induced Crystallization of Amorphous Poly (Lactic Acid) FilmDocumento11 páginasEffects of Various Liquid Organic Solvents On Solvent-Induced Crystallization of Amorphous Poly (Lactic Acid) FilmqueteimportaAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- History of Crime and Criminal Justice in America EditedDocumento7 páginasHistory of Crime and Criminal Justice in America EditedcarolineAinda não há avaliações
- Method Setting Out of Drainage 2Documento9 páginasMethod Setting Out of Drainage 2amin100% (1)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- 6 Human Diseases That Cause by VirusesDocumento7 páginas6 Human Diseases That Cause by VirusesJefry JapAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- NWO Plans Exposed by Insider in 1969Documento36 páginasNWO Plans Exposed by Insider in 1969Stig Dragholm100% (3)
- DICGC - For Depositors - A Guide To Deposit InsuranceDocumento10 páginasDICGC - For Depositors - A Guide To Deposit InsuranceSachinAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Vertical Transportation in BuildingsDocumento46 páginasVertical Transportation in BuildingsHIMA MiniAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Big BazaarDocumento6 páginasBig BazaaraniketsangodcarAinda não há avaliações
- Midas Tutorial Fea 7Documento3 páginasMidas Tutorial Fea 7sasiAinda não há avaliações
- Saep 1160Documento12 páginasSaep 1160JithuJohn100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Using The Time Domain Reflectometer To Check For and Locate A FaultDocumento5 páginasUsing The Time Domain Reflectometer To Check For and Locate A FaultSikandar MasoodAinda não há avaliações
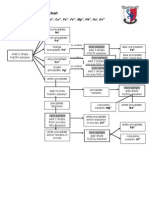
- Testing For Cations Flow ChartDocumento2 páginasTesting For Cations Flow Chartapi-252561013Ainda não há avaliações
- Challenges in The Functional Diagnosis of Thyroid Nodules Before Surgery For TSH-producing Pituitary AdenomaDocumento5 páginasChallenges in The Functional Diagnosis of Thyroid Nodules Before Surgery For TSH-producing Pituitary AdenomaAthul IgnatiusAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Human Nutritional RequirementsDocumento3 páginasHuman Nutritional RequirementsAgnesMagadiaAinda não há avaliações
- Supplementary Spec To API Specification 17D Subsea Wellhead and Tree Equipment With Justifications S 561Jv2022 11Documento81 páginasSupplementary Spec To API Specification 17D Subsea Wellhead and Tree Equipment With Justifications S 561Jv2022 11maximusala83Ainda não há avaliações
- Blotter EntryDocumento2 páginasBlotter EntryCharline Khie Silvestra PortemCamposanoAinda não há avaliações
- MPCA Response 5.29.20Documento2 páginasMPCA Response 5.29.20Duluth News TribuneAinda não há avaliações
- AE Board Review Part3 - MSWord2003 Long Paper 2011Documento12 páginasAE Board Review Part3 - MSWord2003 Long Paper 2011Jan14Ainda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Lipoma in Submandibular Region - A Case ReportDocumento4 páginasLipoma in Submandibular Region - A Case Reportmaxfac2010Ainda não há avaliações
- Static Fluid: It Is Mass Per Unit Volume at Certain TemperatureDocumento11 páginasStatic Fluid: It Is Mass Per Unit Volume at Certain TemperatureMohamed El-GoharyAinda não há avaliações
- Excuse Letter1Documento1 páginaExcuse Letter1Myiel AngelAinda não há avaliações
- CPHQ Text BookDocumento20 páginasCPHQ Text BookCphq Cphq Ali100% (2)