Você também pode gostar
- NCP For FrostbiteDocumento2 páginasNCP For FrostbiteRommar RomeroAinda não há avaliações
- Respiratory Distress SyndromeDocumento4 páginasRespiratory Distress SyndromeRommar RomeroAinda não há avaliações
- NCP For AnaphylacticDocumento3 páginasNCP For AnaphylacticRommar Romero67% (3)
- Scope and Limitation On Thesis Patients Satisfaction On Charity WardDocumento1 páginaScope and Limitation On Thesis Patients Satisfaction On Charity WardRommar RomeroAinda não há avaliações
- Introduction On Thesis Patients Satisfaction On Charity WardDocumento2 páginasIntroduction On Thesis Patients Satisfaction On Charity WardRommar RomeroAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Topic 1 Endocrine SystemDocumento140 páginasTopic 1 Endocrine SystemmasdfgAinda não há avaliações
- Endocrine SystemDocumento3 páginasEndocrine SystemAnne Jillian83% (6)
- Sistem Endokrin 2 - TugasDocumento19 páginasSistem Endokrin 2 - TugasElrisa SalsabillaAinda não há avaliações
- Thyroid Function TestDocumento11 páginasThyroid Function TestBookmyscansAinda não há avaliações
- Hormones:: Signaling MoleculesDocumento20 páginasHormones:: Signaling MoleculesSangeeta DwivediAinda não há avaliações
- The Endocrine System: Regulation of Thyroid Hormone SecretionDocumento24 páginasThe Endocrine System: Regulation of Thyroid Hormone SecretionAndrea PescosolidoAinda não há avaliações
- Breakthrough ANY Weight Loss Plateau WebinarDocumento5 páginasBreakthrough ANY Weight Loss Plateau WebinarIvan SanaderAinda não há avaliações
- Biology Test (Reprod, Endocrine)Documento2 páginasBiology Test (Reprod, Endocrine)eruchAinda não há avaliações
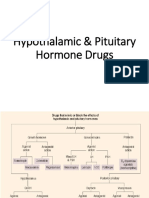
- Hypothalamic & Pituitary Hormone DrugsDocumento29 páginasHypothalamic & Pituitary Hormone DrugsDylan MansillaAinda não há avaliações
- Pathophysio (Case 3)Documento1 páginaPathophysio (Case 3)Carl Michael RazoAinda não há avaliações
- Science 10 A2.2 Pituitary and Hypothalamus The Bodys Control CentersDocumento40 páginasScience 10 A2.2 Pituitary and Hypothalamus The Bodys Control CentersKhobie PabilicoAinda não há avaliações
- Gonadal Hormones and InhibitorsDocumento14 páginasGonadal Hormones and InhibitorsbluesumAinda não há avaliações
- 1167 4889 1 PBDocumento11 páginas1167 4889 1 PBaffan kurniawanAinda não há avaliações
- Introduction of Hormones and Hormone ReceptorsDocumento15 páginasIntroduction of Hormones and Hormone ReceptorsAshraf MahmoudAinda não há avaliações
- Endocrine Surgery MCQ: Precise Diagnostic Screening for Thyroid NodulesDocumento71 páginasEndocrine Surgery MCQ: Precise Diagnostic Screening for Thyroid NodulesShriyansh ChaharAinda não há avaliações
- Blood TSH ReportDocumento1 páginaBlood TSH Reportshilpishukla1191Ainda não há avaliações
- And How They Work: Types of InsulinDocumento1 páginaAnd How They Work: Types of InsulinDea D100% (1)
- Endocrine SystemDocumento28 páginasEndocrine SystemJay Lorie DingsonAinda não há avaliações
- Endocrine Glands and Hormone SignallingDocumento12 páginasEndocrine Glands and Hormone SignallingMohammed EljackAinda não há avaliações
- Chemical Coordination and IntegrationDocumento17 páginasChemical Coordination and IntegrationHemant KumarAinda não há avaliações
- Prevalence and Characteristics of Women With Polycystic Ovary Syndrome in Bangladesh - A Narrative ReviewDocumento10 páginasPrevalence and Characteristics of Women With Polycystic Ovary Syndrome in Bangladesh - A Narrative Reviewnanjiba.khanAinda não há avaliações
- Comparison of Systemic Corticosteroid Preparations - UpToDateDocumento1 páginaComparison of Systemic Corticosteroid Preparations - UpToDateMarco Salinas ContrerasAinda não há avaliações
- NHS FPX 6004 Assessment 2 Policy ProposalDocumento4 páginasNHS FPX 6004 Assessment 2 Policy Proposaljoohnsmith070Ainda não há avaliações
- Posterior Pituitary: DR Axelle Saverettiar Mbbs Physiology Department SSR Medical CollegeDocumento60 páginasPosterior Pituitary: DR Axelle Saverettiar Mbbs Physiology Department SSR Medical CollegeÑäd ÉèmAinda não há avaliações
- Diffuse Thyroid Disease Presentation TorontoDocumento56 páginasDiffuse Thyroid Disease Presentation Torontoرونالين كستروAinda não há avaliações
- Growth Hormone Deficiency - ChildrenDocumento4 páginasGrowth Hormone Deficiency - ChildrenFenita Renny DinataAinda não há avaliações
- (1479683X - European Journal of Endocrinology) DIAGNOSIS of ENDOCRINE DISEASE - How Reliable Are Free Thyroid and Total T3 Hormone AssaysDocumento9 páginas(1479683X - European Journal of Endocrinology) DIAGNOSIS of ENDOCRINE DISEASE - How Reliable Are Free Thyroid and Total T3 Hormone AssaysRaza MuhammadAinda não há avaliações
- Adrenocortical Carcinoma PresentationDocumento21 páginasAdrenocortical Carcinoma Presentationmonday125Ainda não há avaliações
- Jcem 0709Documento20 páginasJcem 0709Rao Rizwan ShakoorAinda não há avaliações
- Radioactive Iodine Therapy (RAI) for HyperthyroidismDocumento6 páginasRadioactive Iodine Therapy (RAI) for HyperthyroidismFirras SalsabilaAinda não há avaliações