Você também pode gostar
- Mei 2019-PneumonieDocumento10 páginasMei 2019-PneumonieAnnisa Caul HasanahAinda não há avaliações
- Cover TupperwareDocumento1 páginaCover TupperwareAnnisa Caul HasanahAinda não há avaliações
- Wim de Jong 613 9. Nelson 10. 11. Arensman RM, Bambini DA. Congenital DiafragmaticDocumento1 páginaWim de Jong 613 9. Nelson 10. 11. Arensman RM, Bambini DA. Congenital DiafragmaticAnnisa Caul HasanahAinda não há avaliações
- Against All Odds - Westlife: Mariah CareyDocumento3 páginasAgainst All Odds - Westlife: Mariah CareyAnnisa Caul HasanahAinda não há avaliações
- Karl LandsteinerDocumento3 páginasKarl LandsteinerAnnisa Caul HasanahAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Resume Charlie Castro 2Documento13 páginasResume Charlie Castro 2JasonV.PanayAinda não há avaliações
- The Story of Our Health MessageDocumento198 páginasThe Story of Our Health MessageRichard Kyalo Kimilu100% (1)
- Surgery Mcqs Along With KeyDocumento8 páginasSurgery Mcqs Along With KeyFaizan Khan100% (3)
- Brand Name - Generic NameDocumento6 páginasBrand Name - Generic Namejonette carataoAinda não há avaliações
- Cord ProlapseDocumento2 páginasCord ProlapseUsman Ali AkbarAinda não há avaliações
- Mercury Poisoning JDocumento27 páginasMercury Poisoning JJomariexOrtizAinda não há avaliações
- Program at A Glance Konas Perdatin Perdici 2019Documento15 páginasProgram at A Glance Konas Perdatin Perdici 2019achmad mustikaAinda não há avaliações
- Woman Undergoes Revolutionary Treatment For Her Lifelong DepressionDocumento2 páginasWoman Undergoes Revolutionary Treatment For Her Lifelong DepressionsarahnorrisAinda não há avaliações
- Adjustment Disorder: Mind MantraDocumento6 páginasAdjustment Disorder: Mind MantraDr. JarrelAinda não há avaliações
- Cardiogenic ShockDocumento27 páginasCardiogenic ShockMuhammad Ikbar100% (1)
- The Parents Guide To Occupational Therapy For Autism and Other Special Needs - NodrmDocumento84 páginasThe Parents Guide To Occupational Therapy For Autism and Other Special Needs - NodrmAimeeUnidadEsguerra100% (1)
- Breathing ExerciseDocumento2 páginasBreathing ExerciseDinesh KumarAinda não há avaliações
- 132 Sensory Diet 090212Documento2 páginas132 Sensory Diet 090212Sally Vesper100% (1)
- LIST OF ENGLISH PUBLICATIONS ( (Alfried Längle)Documento3 páginasLIST OF ENGLISH PUBLICATIONS ( (Alfried Längle)abaeram2Ainda não há avaliações
- Attachment and InterventionDocumento13 páginasAttachment and InterventioneducacionchileAinda não há avaliações
- Handout 1-What Is JSJ & Mudras-1Documento1 páginaHandout 1-What Is JSJ & Mudras-1Gg KAinda não há avaliações
- Fluid Management and Obstetric ShockDocumento188 páginasFluid Management and Obstetric Shocksprimal50% (2)
- Discuss - 1) Aetiology 2) Pathology 3) Diagnosis 4) ManagementDocumento14 páginasDiscuss - 1) Aetiology 2) Pathology 3) Diagnosis 4) ManagementAzizan HannyAinda não há avaliações
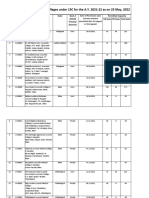
- List of Permitted Ayurveda Colleges For The A.Y. 2021-22 Till 06.05.2022Documento52 páginasList of Permitted Ayurveda Colleges For The A.Y. 2021-22 Till 06.05.2022Re Ed EstAinda não há avaliações
- I.-NCP John Richmond LacadenDocumento3 páginasI.-NCP John Richmond LacadenRichmond Lacaden100% (1)
- Compromised Family Coping NCPDocumento2 páginasCompromised Family Coping NCPJamaeka Gotis100% (1)
- Chapter 5Documento12 páginasChapter 5komalmawra22Ainda não há avaliações
- Onco-Critical Care An Evidence-Based ApproachDocumento539 páginasOnco-Critical Care An Evidence-Based ApproachZuriAinda não há avaliações
- Acute Flaccid ParalysisDocumento4 páginasAcute Flaccid ParalysisZharah RuzAinda não há avaliações
- Lyapko Applicator Eng PDFDocumento23 páginasLyapko Applicator Eng PDFYuldashAinda não há avaliações
- DR SabaDocumento2 páginasDR SabaMuhammad Abrar YousafzaiAinda não há avaliações
- DDH - Slide PresentationDocumento28 páginasDDH - Slide PresentationSheilla RatnasariAinda não há avaliações
- Final ReferencesDocumento29 páginasFinal ReferencesUday KapoorAinda não há avaliações
- Bolus Feeding in Adults A Practical GuideDocumento18 páginasBolus Feeding in Adults A Practical Guideshrutee babraAinda não há avaliações
- Advance Neonatal Procedures Plane ReadyDocumento14 páginasAdvance Neonatal Procedures Plane ReadyKrini TandelAinda não há avaliações