Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Vitamin and Mineral ChartDocumento4 páginasVitamin and Mineral ChartGerarld Immanuel KairupanAinda não há avaliações
- Panduan Pelayanan Medik PB PAPDI 2006Documento418 páginasPanduan Pelayanan Medik PB PAPDI 2006LipatOla12394% (16)
- Vitamin and Mineral ChartDocumento4 páginasVitamin and Mineral ChartGerarld Immanuel KairupanAinda não há avaliações
- Hypothalamus Pituitary Ovarian SystemDocumento10 páginasHypothalamus Pituitary Ovarian SystemAin ZainalAinda não há avaliações
- Soal Ujian Stase Fer 5 April 2021Documento8 páginasSoal Ujian Stase Fer 5 April 2021Bella DirkAinda não há avaliações
- Men's Physique CyclesDocumento1 páginaMen's Physique CyclessahilAinda não há avaliações
- Pro CyclesDocumento7 páginasPro Cyclestselentisharris15867% (3)
- Guias Hipertension 2023 EscDocumento199 páginasGuias Hipertension 2023 Escmiguel contrerasAinda não há avaliações
- 8 Health Laws PDFDocumento2 páginas8 Health Laws PDFGerarld Immanuel KairupanAinda não há avaliações
- TugasDocumento60 páginasTugasGerarld Immanuel KairupanAinda não há avaliações
- HydrotherapyDocumento208 páginasHydrotherapyGerarld Immanuel KairupanAinda não há avaliações
- The Principles of Good HealthDocumento2 páginasThe Principles of Good HealthGerarld Immanuel KairupanAinda não há avaliações
- DEPKES RI NEW Pedoman Nasional Penanggulangan TBC 2011Documento110 páginasDEPKES RI NEW Pedoman Nasional Penanggulangan TBC 2011familyman8091% (11)
- Natural Remedies: HydrotherapyDocumento5 páginasNatural Remedies: HydrotherapyGerarld Immanuel KairupanAinda não há avaliações
- 2018 Wop Combined No PhotosDocumento107 páginas2018 Wop Combined No PhotosGerarld Immanuel KairupanAinda não há avaliações
- Focused Abdominal Sonography For Trauma (Fast) - Dr. BunyaminDocumento30 páginasFocused Abdominal Sonography For Trauma (Fast) - Dr. BunyaminGerarld Immanuel KairupanAinda não há avaliações
- Fever and Rash by DR Djatnika (2 September 2014)Documento67 páginasFever and Rash by DR Djatnika (2 September 2014)Gerarld Immanuel KairupanAinda não há avaliações
- Etq118 09Documento13 páginasEtq118 09Gerarld Immanuel KairupanAinda não há avaliações
- Etq118 09Documento13 páginasEtq118 09Gerarld Immanuel KairupanAinda não há avaliações
- Metabolic Era in Ischemic Heart DiseaseDocumento24 páginasMetabolic Era in Ischemic Heart DiseaseGerarld Immanuel KairupanAinda não há avaliações
- Health Message & GospelDocumento13 páginasHealth Message & GospelGerarld Immanuel KairupanAinda não há avaliações
- Light Bearers 2012 Yearend ReportDocumento11 páginasLight Bearers 2012 Yearend ReportGerarld Immanuel KairupanAinda não há avaliações
- Infeksi in Pregnancy and PuerperiumDocumento35 páginasInfeksi in Pregnancy and PuerperiumGerarld Immanuel KairupanAinda não há avaliações
- Incomplete AbortionDocumento37 páginasIncomplete AbortionGerarld Immanuel Kairupan100% (1)
- 8 Health Laws PDFDocumento2 páginas8 Health Laws PDFGerarld Immanuel KairupanAinda não há avaliações
- Anamnesia Fisiatris EditedDocumento47 páginasAnamnesia Fisiatris EditedMuhammad Cahara AdhiAinda não há avaliações
- Natural Remedies: HydrotherapyDocumento5 páginasNatural Remedies: HydrotherapyGerarld Immanuel KairupanAinda não há avaliações
- Anamnesia Fisiatris EditedDocumento47 páginasAnamnesia Fisiatris EditedMuhammad Cahara AdhiAinda não há avaliações
- Crispin, CasmerDocumento2 páginasCrispin, CasmerGerarld Immanuel KairupanAinda não há avaliações
- 8 Health Laws PDFDocumento2 páginas8 Health Laws PDFGerarld Immanuel KairupanAinda não há avaliações
- Bernabe, BenignoDocumento4 páginasBernabe, BenignoGerarld Immanuel KairupanAinda não há avaliações
- Alone: Justification by FaithDocumento13 páginasAlone: Justification by FaithGerarld Immanuel KairupanAinda não há avaliações
- Dela Cruz, ElsaDocumento4 páginasDela Cruz, ElsaGerarld Immanuel KairupanAinda não há avaliações
- Republic of The Philippines Department of Health Baguio General Hospital and Medical Center Psychiatry Department Baguio CityDocumento3 páginasRepublic of The Philippines Department of Health Baguio General Hospital and Medical Center Psychiatry Department Baguio CityGerarld Immanuel KairupanAinda não há avaliações
- New Estrogen and ProgesteroneDocumento56 páginasNew Estrogen and ProgesteroneHBrAinda não há avaliações
- Embryo Transfer: Abdul Samik Department of Veterinary Reproduction Faculty of Veterinary Medicine - UnairDocumento80 páginasEmbryo Transfer: Abdul Samik Department of Veterinary Reproduction Faculty of Veterinary Medicine - UnairNita AndriyanAinda não há avaliações
- Viva Level Endocrine MCQ 1Documento1 páginaViva Level Endocrine MCQ 1imnnayakAinda não há avaliações
- Sankha Jee Medical Receipt-18.08.2022Documento12 páginasSankha Jee Medical Receipt-18.08.2022saajnaAinda não há avaliações
- Gonadal Hormones and InhibitorsDocumento14 páginasGonadal Hormones and InhibitorsbluesumAinda não há avaliações
- COBAS 6000: E601 Reagent Inventory MONTH/YEARDocumento2 páginasCOBAS 6000: E601 Reagent Inventory MONTH/YEARCharmaine Corpuz GranilAinda não há avaliações
- COBAS 6000: E601 Reagent Inventory MONTH/YEAR: - AUGUST 2020Documento3 páginasCOBAS 6000: E601 Reagent Inventory MONTH/YEAR: - AUGUST 2020Charmaine Corpuz GranilAinda não há avaliações
- Pl-Tosoh-Maret 2020Documento3 páginasPl-Tosoh-Maret 2020Labkesda Kota BaubauAinda não há avaliações
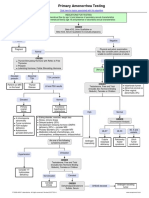
- Primary Amenorrhea Testing AlgorithmDocumento1 páginaPrimary Amenorrhea Testing AlgorithmfarmasiAinda não há avaliações
- CDGP Versus HypogonadismDocumento25 páginasCDGP Versus HypogonadismmpintobAinda não há avaliações
- An A Boli ZantesDocumento3 páginasAn A Boli Zantesvinigoncalves275Ainda não há avaliações
- Sub: Price List of Minividas Reagents and ConsumablesDocumento3 páginasSub: Price List of Minividas Reagents and ConsumablesChemudupati BharaniAinda não há avaliações
- Gonadal Hormones and InhibitorsDocumento101 páginasGonadal Hormones and Inhibitors2012100% (4)
- Total Estradiol LectureDocumento68 páginasTotal Estradiol LectureLucas ElyAinda não há avaliações
- In-SeT 5E Lesson PlanDocumento29 páginasIn-SeT 5E Lesson Planaiza arcilloAinda não há avaliações
- Female Precocious Puberty AlgorithmDocumento1 páginaFemale Precocious Puberty AlgorithmRICHI ADITYAAinda não há avaliações
- Chemical Coordination and Integration NotesDocumento22 páginasChemical Coordination and Integration Notesarshi27khan3057Ainda não há avaliações
- BODYTECH Price-1Documento1 páginaBODYTECH Price-1nk4xp5ds6rAinda não há avaliações
- Lista de Sustancias 2020 DistribuidorDocumento15 páginasLista de Sustancias 2020 DistribuidorRafael ValdezAinda não há avaliações
- 2 Nurfadilah 3Documento9 páginas2 Nurfadilah 3Khalid Hidayat Al IkhsanAinda não há avaliações
- Follicle-Stimulating Hormone: Glycoprotein Hormones, Alpha PolypeptideDocumento6 páginasFollicle-Stimulating Hormone: Glycoprotein Hormones, Alpha PolypeptideNTA UGC-NETAinda não há avaliações
- Reproductive Pharmacology Lecturio ReflectionDocumento7 páginasReproductive Pharmacology Lecturio ReflectionNathaniel SolisAinda não há avaliações
- Precocious PubertyDocumento13 páginasPrecocious PubertyLee Woan ChyiAinda não há avaliações
- Lyphochek Immunoassay Plus Control Levels 1, 2 and 3: Revision Date 2020-06-29 Indicates Revised InformationDocumento2 páginasLyphochek Immunoassay Plus Control Levels 1, 2 and 3: Revision Date 2020-06-29 Indicates Revised InformationMDD Engineering100% (2)
- Reference Ranges Pediatric Endocrin PDFDocumento14 páginasReference Ranges Pediatric Endocrin PDFshoratanAinda não há avaliações
- Julho - 22 Us CoachDocumento7 páginasJulho - 22 Us CoachPantajr - GTR250Ainda não há avaliações