Você também pode gostar
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Instant Healing Meditation (Basic) - David Alan RamsdaleDocumento31 páginasInstant Healing Meditation (Basic) - David Alan Ramsdaledeichem88% (8)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Chronic Obstructive Pulmonary DiseaseDocumento36 páginasChronic Obstructive Pulmonary DiseaseHazel ManuelAinda não há avaliações
- Acute AbdomenDocumento122 páginasAcute AbdomenJunayed Safar MahmudAinda não há avaliações
- 2021-08-16 MD Anderson RecordsDocumento83 páginas2021-08-16 MD Anderson RecordsjeffreybodinAinda não há avaliações
- Emergency Response Drill Scenarios 1Documento10 páginasEmergency Response Drill Scenarios 1Arfiyunanto Malika50% (4)
- Precautionary and Sanitary Practices in Handling FoodDocumento31 páginasPrecautionary and Sanitary Practices in Handling FoodBrenNan ChannelAinda não há avaliações
- Chapter 32 - Stop-Controlled Intersections Supp - 600Documento74 páginasChapter 32 - Stop-Controlled Intersections Supp - 600Ana María Lira CastroAinda não há avaliações
- Al-Hijamah (Cupping) - Healing The Sunnah Way - Amjad Ahsan AliDocumento194 páginasAl-Hijamah (Cupping) - Healing The Sunnah Way - Amjad Ahsan Alihal bannaAinda não há avaliações
- Case Study On Gastric Outlet ObstructionDocumento37 páginasCase Study On Gastric Outlet ObstructionJunayed Safar Mahmud100% (4)
- Introduction To Endocrinology & Endocrine Function Tests.Documento14 páginasIntroduction To Endocrinology & Endocrine Function Tests.Junayed Safar MahmudAinda não há avaliações
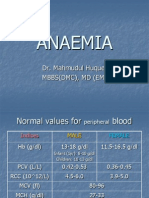
- Anaemia: Dr. Mahmudul Huque. Mbbs (DMC), MD (Em)Documento32 páginasAnaemia: Dr. Mahmudul Huque. Mbbs (DMC), MD (Em)Junayed Safar MahmudAinda não há avaliações
- Jadwal Praktek Dokter Spesialis Baru 1akreditasi AllDocumento8 páginasJadwal Praktek Dokter Spesialis Baru 1akreditasi Alldonny suryaAinda não há avaliações
- Chapter Review: True or FalseDocumento2 páginasChapter Review: True or FalseJames Gabriel SalardaAinda não há avaliações
- Global Developmental DelayDocumento2 páginasGlobal Developmental DelayAtlerAinda não há avaliações
- Mechanical Ventilation 2015Documento18 páginasMechanical Ventilation 2015Nauman GilaniAinda não há avaliações
- Patient Medical Records: Discharge and Home-Care InstructionsDocumento27 páginasPatient Medical Records: Discharge and Home-Care InstructionsAnamaria ManceraAinda não há avaliações
- Islamic Method of Slaughtering Animals Is BetterDocumento2 páginasIslamic Method of Slaughtering Animals Is Betterapi-26133437Ainda não há avaliações
- An Analytical Study of Euthanasia in India With - Rucha Kulkarni PDFDocumento150 páginasAn Analytical Study of Euthanasia in India With - Rucha Kulkarni PDFDazzler AshishAinda não há avaliações
- Mendiguchia 2012 Rectus Femoris Muscle Injuries in Football-A Clinically Relevant Review of Mechanisms of Injury, Risk Factors and Preventive Strategies PDFDocumento11 páginasMendiguchia 2012 Rectus Femoris Muscle Injuries in Football-A Clinically Relevant Review of Mechanisms of Injury, Risk Factors and Preventive Strategies PDFJuan PalomoAinda não há avaliações
- عملیات شفاء امراض Amliyat Shifa Amraz 0091-33-23607502 - DIL KE AMRAZ KA RUHANI ELAJ (Spiritual Treatment of Heart Diseases)Documento4 páginasعملیات شفاء امراض Amliyat Shifa Amraz 0091-33-23607502 - DIL KE AMRAZ KA RUHANI ELAJ (Spiritual Treatment of Heart Diseases)msmpaki@yahoo.comAinda não há avaliações
- PhilHealth Circular 35 S. 2013 PDFDocumento17 páginasPhilHealth Circular 35 S. 2013 PDFNomad's CastleAinda não há avaliações
- Daftar Pustaka OaDocumento2 páginasDaftar Pustaka OaCut Naja SoviaAinda não há avaliações
- Read The Text and Answer Questions 5 and 6.: Cookbook. New York: DK Publishing, 2007, P. 8Documento1 páginaRead The Text and Answer Questions 5 and 6.: Cookbook. New York: DK Publishing, 2007, P. 8matheus gonçalvesAinda não há avaliações
- MLP by StateDocumento12 páginasMLP by StateFlor OMAinda não há avaliações
- Orthodontic Appliances: General Requirements of An Orthodontic ApplianceDocumento20 páginasOrthodontic Appliances: General Requirements of An Orthodontic ApplianceSafaa GhobAinda não há avaliações
- Movie ReviewDocumento5 páginasMovie ReviewVangeline MandiitAinda não há avaliações
- Advise Patients Not To Exceed The Recommended Dose or Frequency of AdministrationDocumento3 páginasAdvise Patients Not To Exceed The Recommended Dose or Frequency of AdministrationPrincess M Viznar BalolotAinda não há avaliações
- Discharge Planning: MedicationDocumento3 páginasDischarge Planning: MedicationLeasAinda não há avaliações
- BIS A2000 - Operating ManualDocumento102 páginasBIS A2000 - Operating Manualgabygg06Ainda não há avaliações
- MollyDocumento7 páginasMollyapi-534233456Ainda não há avaliações
- Pain Management: Dr. Prabowo Wicaksono Span Bagian/Smf Anestesi FK Unissula/Rsisa 2007Documento27 páginasPain Management: Dr. Prabowo Wicaksono Span Bagian/Smf Anestesi FK Unissula/Rsisa 2007Fendy PrasetyoAinda não há avaliações
- DiphtheriaDocumento11 páginasDiphtheriabrigde_xAinda não há avaliações
- Genetic Engineering Applications in Animal BreedingDocumento6 páginasGenetic Engineering Applications in Animal BreedingFadilla HadiwijayaAinda não há avaliações
- Ezhilan MBADocumento48 páginasEzhilan MBAVigneshMuchiAinda não há avaliações