Você também pode gostar
- Programs and Projects in The National SettingDocumento58 páginasPrograms and Projects in The National SettingAnn Grethel Tan100% (1)
- Antenatal Care Services: by DR - Chinedu Ibeh Thursday, 16 APRIL 2015Documento81 páginasAntenatal Care Services: by DR - Chinedu Ibeh Thursday, 16 APRIL 2015SehaRizaAinda não há avaliações
- Heavy Menstrual BleedingDocumento29 páginasHeavy Menstrual BleedingsanjupainAinda não há avaliações
- Fundal Height ScreeningDocumento10 páginasFundal Height ScreeningDr_Soranus100% (1)
- Postterm Pregnancy Risks & Management OptionsDocumento5 páginasPostterm Pregnancy Risks & Management OptionsOmar MohammedAinda não há avaliações
- Management of Pregnant PatientDocumento113 páginasManagement of Pregnant PatientWilliam BharathAinda não há avaliações
- Physical Examination For Pregnant WomanDocumento31 páginasPhysical Examination For Pregnant WomanFrancia ToledanoAinda não há avaliações
- Integrated Management of Childhood IllnessDocumento3 páginasIntegrated Management of Childhood IllnessJanine Alexis BuenviajeAinda não há avaliações
- Geriatric Giants Iwal 1 2020Documento58 páginasGeriatric Giants Iwal 1 2020selymariaAinda não há avaliações
- Safe Motherhood: Reproductive Health I Clinical Medicine ClassDocumento32 páginasSafe Motherhood: Reproductive Health I Clinical Medicine Classmoreen kipkemoiAinda não há avaliações
- Emetics and Antiemetics DrugsDocumento15 páginasEmetics and Antiemetics DrugsrajenderAinda não há avaliações
- Integrated Management of Childhood IllnessDocumento52 páginasIntegrated Management of Childhood IllnessRitz CelsoAinda não há avaliações
- DOT for TB Treatment: Minnesota Health Dept GuideDocumento2 páginasDOT for TB Treatment: Minnesota Health Dept Guideahsanraja123Ainda não há avaliações
- Haematinic DeficienciesDocumento7 páginasHaematinic DeficienciesFrancesca Li100% (1)
- Elements of Primary Health CareDocumento4 páginasElements of Primary Health CareJAY LAPAZ ANDRES, RN, BSN, MAN (C), MAEd.. (C)Ainda não há avaliações
- Peptic Ulcer Disease: Causes, Symptoms and TreatmentDocumento60 páginasPeptic Ulcer Disease: Causes, Symptoms and TreatmentNehimyaAinda não há avaliações
- Anemia in Pregnancy GuideDocumento7 páginasAnemia in Pregnancy GuideLenrok AdrianAinda não há avaliações
- Diagnosis and Management of ADRsDocumento45 páginasDiagnosis and Management of ADRspriyankaAinda não há avaliações
- Research-Proposal MaeDocumento6 páginasResearch-Proposal MaeJester RafolsAinda não há avaliações
- Pharmacology Mock Exam MCQDocumento8 páginasPharmacology Mock Exam MCQanaeshklAinda não há avaliações
- Food FortificationDocumento11 páginasFood FortificationRekha G.Ainda não há avaliações
- Case Study On Breast EngorgementDocumento2 páginasCase Study On Breast Engorgementaxexrxdxnxaxs zxexlxaxzxnxoxgAinda não há avaliações
- Home VisitDocumento22 páginasHome Visitenam professorAinda não há avaliações
- Assessment of Digestive and Gastrointestinal FunctionDocumento19 páginasAssessment of Digestive and Gastrointestinal FunctionMarichelle Vicente- Delos SantosAinda não há avaliações
- Oral Glucose Tolerance TestDocumento4 páginasOral Glucose Tolerance TestCyna Jane Yao AlcularAinda não há avaliações
- Etat + PDFDocumento56 páginasEtat + PDFShandy BAinda não há avaliações
- Mod Family Planning Final PDFDocumento124 páginasMod Family Planning Final PDFPatricia Anne EsmedillaAinda não há avaliações
- BathingDocumento34 páginasBathingshannon c. lewisAinda não há avaliações
- Module 2.2 - Concept of EBP PDFDocumento24 páginasModule 2.2 - Concept of EBP PDFvincyAinda não há avaliações
- LeukorrheaDocumento29 páginasLeukorrheaThorsang Chayovan100% (1)
- Emergency Contraception and Emergency Contraceptive Pills (ECPs)Documento39 páginasEmergency Contraception and Emergency Contraceptive Pills (ECPs)cafemed100% (1)
- CP ON PUD (1) ADocumento20 páginasCP ON PUD (1) ADeekshitha DanthuluriAinda não há avaliações
- Case StudyDocumento48 páginasCase Studysimbarashe tangwadzanaAinda não há avaliações
- Emeset MedicalDocumento16 páginasEmeset MedicalSwapnil PatilAinda não há avaliações
- 24 - Family PlanningDocumento88 páginas24 - Family PlanningGabrielle CatalanAinda não há avaliações
- Lecture Notes On AphDocumento41 páginasLecture Notes On AphEyob MizanAinda não há avaliações
- Nutritional Status of School Age Children in Private Elementary Schools: Basis For A Proposed Meal Management PlanDocumento5 páginasNutritional Status of School Age Children in Private Elementary Schools: Basis For A Proposed Meal Management PlanIjaems JournalAinda não há avaliações
- The Philippine Health Care SystemDocumento3 páginasThe Philippine Health Care SystemMiki TroyoAinda não há avaliações
- Headss For AdolescentsDocumento7 páginasHeadss For AdolescentsSamer FarhanAinda não há avaliações
- Importance of Complementary FeedingDocumento6 páginasImportance of Complementary FeedingJethro Floyd QuintoAinda não há avaliações
- Essential Update: Pediatric Pneumonia May Be Effectively Treated With Twice-Daily AmoxicillinDocumento54 páginasEssential Update: Pediatric Pneumonia May Be Effectively Treated With Twice-Daily AmoxicillinYostesara Maurena SantosaAinda não há avaliações
- FAMILY PLANNING PROGRAM HandoutsDocumento2 páginasFAMILY PLANNING PROGRAM HandoutsWilma Nierva BeraldeAinda não há avaliações
- 4 - Hormonal ContraceptivesDocumento109 páginas4 - Hormonal ContraceptivesNoskcire OremorAinda não há avaliações
- Maternity Nursing Course Outline - Clinical PDFDocumento24 páginasMaternity Nursing Course Outline - Clinical PDFAshraf NoriAinda não há avaliações
- B SC Nursing Syllabus INC PDFDocumento183 páginasB SC Nursing Syllabus INC PDFsohini bhattacharyaAinda não há avaliações
- Practice Guidelines: For Family PhysiciansDocumento0 páginaPractice Guidelines: For Family PhysiciansMuhammad GoharAinda não há avaliações
- 3 ConstipationDocumento18 páginas3 Constipationكسلان اكتب اسميAinda não há avaliações
- Basic Public Health (1) - MergedDocumento89 páginasBasic Public Health (1) - Mergedrimsha tariqAinda não há avaliações
- Nutrition Lecture PowerpointDocumento247 páginasNutrition Lecture PowerpointRenz ReyesAinda não há avaliações
- Prostaglandins: Hormone-Like Substances With Diverse Physiological RolesDocumento21 páginasProstaglandins: Hormone-Like Substances With Diverse Physiological RolesaneenaAinda não há avaliações
- Causes, Symptoms and Treatments of VaginitisDocumento16 páginasCauses, Symptoms and Treatments of VaginitisMae Christelle Hamoy100% (2)
- Case Scenario #4 (Postpartum)Documento3 páginasCase Scenario #4 (Postpartum)Krizzia Angela BacotocAinda não há avaliações
- Macro and Micro MineralsDocumento54 páginasMacro and Micro MineralsTrish LeonardoAinda não há avaliações
- Report On Family Planning (4400)Documento27 páginasReport On Family Planning (4400)Bikram KushaalAinda não há avaliações
- Health Assessment in Nursing (LEC) : Prepared By: Mark Joseph V. Liwanag, RN, MSNDocumento43 páginasHealth Assessment in Nursing (LEC) : Prepared By: Mark Joseph V. Liwanag, RN, MSNCj MayoyoAinda não há avaliações
- Mers Cov/H1N1/Corona Virus: By: Gilbert B. Gelig IIDocumento25 páginasMers Cov/H1N1/Corona Virus: By: Gilbert B. Gelig IIDaciel GleeAinda não há avaliações
- Anc Inc PNCDocumento29 páginasAnc Inc PNCDrArun SinghAinda não há avaliações
- Pregnancy Health Guide - 40 Tips for a Safe PregnancyDocumento18 páginasPregnancy Health Guide - 40 Tips for a Safe PregnancyNada MotahharAinda não há avaliações
- Cyanosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandCyanosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNota: 5 de 5 estrelas5/5 (1)
- Swollen Kidney, (Hydronephrosis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandSwollen Kidney, (Hydronephrosis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Isolated Glomerular Disease With Recurrent Gross HematuriaDocumento17 páginasIsolated Glomerular Disease With Recurrent Gross HematuriaArun GeorgeAinda não há avaliações
- Febrile Neutropenia Esmo PDFDocumento8 páginasFebrile Neutropenia Esmo PDFArun GeorgeAinda não há avaliações
- Febrile Neutropenia ArunDocumento40 páginasFebrile Neutropenia ArunArun GeorgeAinda não há avaliações
- X-rays in Pediatrics: A Concise Guide to Common FindingsDocumento111 páginasX-rays in Pediatrics: A Concise Guide to Common FindingsArun GeorgeAinda não há avaliações
- Statistics For OsceDocumento77 páginasStatistics For OsceArun GeorgeAinda não há avaliações
- Paediatric Chest X-RayDocumento10 páginasPaediatric Chest X-RayIdha KurniasihAinda não há avaliações
- X Rays EssentialsDocumento48 páginasX Rays EssentialsArun GeorgeAinda não há avaliações
- Electrolytes OsmolalityDocumento48 páginasElectrolytes OsmolalityArun GeorgeAinda não há avaliações
- Diagnostic Test 1Documento4 páginasDiagnostic Test 1aryawiraAinda não há avaliações
- Membranous GlomerulopathyDocumento10 páginasMembranous GlomerulopathyArun GeorgeAinda não há avaliações
- Approach To HematuriaDocumento45 páginasApproach To HematuriaArun GeorgeAinda não há avaliações
- Rapidly Progressive Glomerulonephritis (RPGN): Causes, Symptoms, DiagnosisDocumento13 páginasRapidly Progressive Glomerulonephritis (RPGN): Causes, Symptoms, DiagnosisArun GeorgeAinda não há avaliações
- Fluids and Electrolytes in Pediatrics FinalDocumento41 páginasFluids and Electrolytes in Pediatrics FinalArun GeorgeAinda não há avaliações
- Understanding Membranoproliferative Glomerulonephritis (MPGNDocumento10 páginasUnderstanding Membranoproliferative Glomerulonephritis (MPGNArun GeorgeAinda não há avaliações
- HematuriaDocumento13 páginasHematuriaArun GeorgeAinda não há avaliações
- Other Chronic InfectionDocumento6 páginasOther Chronic InfectionArun GeorgeAinda não há avaliações
- Acute Poststreptococcal Glomerulonephritis (APSGNDocumento16 páginasAcute Poststreptococcal Glomerulonephritis (APSGNArun GeorgeAinda não há avaliações
- DermDocumento62 páginasDermArun GeorgeAinda não há avaliações
- SleDocumento11 páginasSleArun GeorgeAinda não há avaliações
- HSPDocumento7 páginasHSPArun GeorgeAinda não há avaliações
- Safety and PreventionDocumento17 páginasSafety and PreventionArun GeorgeAinda não há avaliações
- Glomerular DiseasesDocumento24 páginasGlomerular DiseasesArun GeorgeAinda não há avaliações
- Report of National Consultation On Diagnosis and Treatment of Pediatric TBDocumento27 páginasReport of National Consultation On Diagnosis and Treatment of Pediatric TBArun GeorgeAinda não há avaliações
- IemDocumento80 páginasIemArun GeorgeAinda não há avaliações
- Resuscitation Team ConceptDocumento7 páginasResuscitation Team ConceptArun GeorgeAinda não há avaliações
- Infectious DiseasesDocumento98 páginasInfectious DiseasesArun GeorgeAinda não há avaliações
- Lecture For Medical Students-DevelopmentDocumento7 páginasLecture For Medical Students-DevelopmentArun GeorgeAinda não há avaliações
- Body Fluids and Fluid TherapyDocumento43 páginasBody Fluids and Fluid TherapyArun GeorgeAinda não há avaliações
- ImmunizationDocumento45 páginasImmunizationArun GeorgeAinda não há avaliações
- CnsDocumento15 páginasCnsArun GeorgeAinda não há avaliações
- Strategies in Teaching Social Studies Inductive and Deductive Andragogy vs. PedagogyDocumento31 páginasStrategies in Teaching Social Studies Inductive and Deductive Andragogy vs. PedagogyArvie VillegasAinda não há avaliações
- Gen EdDocumento16 páginasGen EdErika Joy Pacate LatojaAinda não há avaliações
- Thomas McPherson Brown MD Treatment of Rheumatoid DiseaseDocumento29 páginasThomas McPherson Brown MD Treatment of Rheumatoid DiseaseLidia Lidia100% (1)
- Default Password For All TMNet Streamyx Supported ModemDocumento2 páginasDefault Password For All TMNet Streamyx Supported ModemFrankly F. ChiaAinda não há avaliações
- HP Police Constable Question Paper 2015Documento9 páginasHP Police Constable Question Paper 2015Rajat SharmãAinda não há avaliações
- Peplink Balance v6.1.2 User ManualDocumento258 páginasPeplink Balance v6.1.2 User ManualoscarledesmaAinda não há avaliações
- Sports Project BbaDocumento10 páginasSports Project Bbadonboy004Ainda não há avaliações
- Acc6475 2721Documento4 páginasAcc6475 2721pak manAinda não há avaliações
- GKB Data Analytics Mandate Part 2Documento9 páginasGKB Data Analytics Mandate Part 2Vilma TejadaAinda não há avaliações
- AppoloDocumento2 páginasAppoloRishabh Madhu SharanAinda não há avaliações
- Database Design Term Project 1Documento3 páginasDatabase Design Term Project 1MuskanAinda não há avaliações
- El 114 The-Adventures-of-Tom-Sawyer-by-Mark-TwainDocumento11 páginasEl 114 The-Adventures-of-Tom-Sawyer-by-Mark-TwainGhreniel V. Benecito100% (1)
- ISO 15184 Paint Hardness TesterDocumento6 páginasISO 15184 Paint Hardness TesterAvinash SilimkarAinda não há avaliações
- 2015 - Product Keys For Autodesk ProductsDocumento7 páginas2015 - Product Keys For Autodesk ProductsmonkeyDivanAinda não há avaliações
- Assertive CommunicationDocumento5 páginasAssertive CommunicationAditi VaidAinda não há avaliações
- Consumer Behavior Study of Two-Wheeler Users in Nasik DistrictDocumento45 páginasConsumer Behavior Study of Two-Wheeler Users in Nasik DistrictHemant ChavanAinda não há avaliações
- Pushover Analysis As Per EC8Documento23 páginasPushover Analysis As Per EC8mihaitimofteAinda não há avaliações
- Copyright WorksheetDocumento3 páginasCopyright WorksheetJADEN GOODWINAinda não há avaliações
- q2 w6 Asteroids Comets MeteorsDocumento61 páginasq2 w6 Asteroids Comets MeteorsxenarealeAinda não há avaliações
- A Complete List of Books On Mead MakingDocumento3 páginasA Complete List of Books On Mead MakingVictor Sá100% (1)
- Karlle Louis P. Obviar - S11-04Documento2 páginasKarlle Louis P. Obviar - S11-04Karlle ObviarAinda não há avaliações
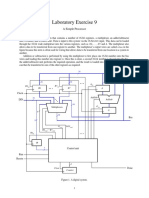
- Laboratory Exercise 9: A Simple ProcessorDocumento8 páginasLaboratory Exercise 9: A Simple ProcessorhxchAinda não há avaliações
- VERTICAL CYLINDRICAL VESSEL WITH FLANGED FLAT TOP AND BOTTOMDocumento1 páginaVERTICAL CYLINDRICAL VESSEL WITH FLANGED FLAT TOP AND BOTTOMsandesh sadvilkarAinda não há avaliações
- CSR FinalDocumento44 páginasCSR FinalrohanAinda não há avaliações
- Clay Minerals Including Related Phyllosilicates: Interdisciplinary Research and Inward IntegrationDocumento16 páginasClay Minerals Including Related Phyllosilicates: Interdisciplinary Research and Inward Integrationbashir DarAinda não há avaliações
- Legal CapacityDocumento7 páginasLegal CapacityAreej UmerAinda não há avaliações
- Inclusion/Exclusion PrincipleDocumento6 páginasInclusion/Exclusion Principlekeelia1saAinda não há avaliações
- AirOS 3.4 - Ubiquiti Wiki#BasicWirelessSettings#BasicWirelessSettingsDocumento24 páginasAirOS 3.4 - Ubiquiti Wiki#BasicWirelessSettings#BasicWirelessSettingsAusAinda não há avaliações
- Engineering Economics - Solution Manual (Chapter 1)Documento1 páginaEngineering Economics - Solution Manual (Chapter 1)Diego GuineaAinda não há avaliações
- 3 Strategic CapabilitiesDocumento20 páginas3 Strategic CapabilitiesMariyam HamdhaAinda não há avaliações