Você também pode gostar
- PHLEBOTOMYDocumento80 páginasPHLEBOTOMYedwineiou100% (4)
- Phlebotomy ReportDocumento40 páginasPhlebotomy ReportJanine Stephanie Hubilla Dela100% (1)
- Phlebotomy Reminders By: Eugene VillanuevaDocumento5 páginasPhlebotomy Reminders By: Eugene VillanuevaNix BatallerAinda não há avaliações
- Blood Collection Procedure (Venipuncture) 07Documento6 páginasBlood Collection Procedure (Venipuncture) 07ridafAinda não há avaliações
- Phlebotomy Lab 1Documento34 páginasPhlebotomy Lab 1Iris Barrera100% (1)
- Phlebotomy Review Shee1Documento8 páginasPhlebotomy Review Shee1Mohammad Usman Qureshi100% (1)
- Hiv, Hepa C: Lab Test Ordered Order Received Prepare The Necessary Things To Be UsedDocumento7 páginasHiv, Hepa C: Lab Test Ordered Order Received Prepare The Necessary Things To Be UsedmaineAinda não há avaliações
- Intro Specimen Collection - PPTX (Autosaved)Documento8 páginasIntro Specimen Collection - PPTX (Autosaved)Vina A. TugasAinda não há avaliações
- Specimen Collection PDFDocumento33 páginasSpecimen Collection PDFadadan100% (1)
- PhlebotomyDocumento183 páginasPhlebotomyFadhli AhmadAinda não há avaliações
- COLLECTION OF BLOOD SPECIMENS MANUAL 2018-2020 - For Lab Guide PDFDocumento27 páginasCOLLECTION OF BLOOD SPECIMENS MANUAL 2018-2020 - For Lab Guide PDFGonzalez ArturoAinda não há avaliações
- Phlebotomy LessonDocumento5 páginasPhlebotomy LessonCaesar Anthony Yuson-Tagalog SanchezAinda não há avaliações
- Week 1 Pmls2Documento45 páginasWeek 1 Pmls2Dayledaniel SorvetoAinda não há avaliações
- Phlebotomy: by Group 1 Cejas, Lequerica, Zambrano, Milian, Joseph NMT 1312 MarshelDocumento48 páginasPhlebotomy: by Group 1 Cejas, Lequerica, Zambrano, Milian, Joseph NMT 1312 MarshelZeeshan Yousuf100% (4)
- 2 PhlebotomyDocumento102 páginas2 PhlebotomyCatherine Merilleno100% (1)
- Blood CollectionDocumento42 páginasBlood CollectionArslan Arshad100% (1)
- Collection of Blood Specimens Manual 2018-2020 - For Lab GuideDocumento27 páginasCollection of Blood Specimens Manual 2018-2020 - For Lab GuideKey SerrAinda não há avaliações
- Phlebotomy: by Group 1 Cejas, Lequerica, Zambrano, Milian, Joseph NMT 1312 MarshelDocumento48 páginasPhlebotomy: by Group 1 Cejas, Lequerica, Zambrano, Milian, Joseph NMT 1312 Marshelkriss Wong100% (1)
- Pre-Analytical Consideration and Venipuncture ComplicationsDocumento52 páginasPre-Analytical Consideration and Venipuncture ComplicationsVenom100% (1)
- Objectives: Pre-Analytical Considerations in PhlebotomyDocumento9 páginasObjectives: Pre-Analytical Considerations in PhlebotomyMr. Potatohead100% (1)
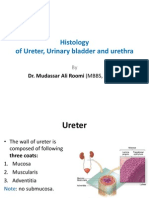
- Histology of Ureter, Urinary Bladder and Urethra by Dr. RoomiDocumento20 páginasHistology of Ureter, Urinary Bladder and Urethra by Dr. RoomiMudassar Roomi100% (4)
- Blood and Blood Components-LectureDocumento12 páginasBlood and Blood Components-LectureSj EclipseAinda não há avaliações
- Phlebotomy ResumeDocumento2 páginasPhlebotomy Resumeapi-452914737Ainda não há avaliações
- Pre-Analytical Laboratory ErrorsDocumento26 páginasPre-Analytical Laboratory ErrorskillerkraitAinda não há avaliações
- PhlebotomyDocumento25 páginasPhlebotomyayoonia100% (1)
- Complications To PhlebotomyDocumento4 páginasComplications To Phlebotomybenrmt67% (3)
- Understanding PhlebotomyDocumento4 páginasUnderstanding PhlebotomyAngelo Jude CumpioAinda não há avaliações
- HS CLT 3 TheRoleOfAPhlebotomistPowerPointDocumento19 páginasHS CLT 3 TheRoleOfAPhlebotomistPowerPointtapan_tsgAinda não há avaliações
- PhlebDocumento44 páginasPhlebCharmeigne CaronanAinda não há avaliações
- PhlebotomyDocumento37 páginasPhlebotomykreatura5100% (2)
- Transfusion of Blood & Blood Components1Documento45 páginasTransfusion of Blood & Blood Components1Chamika Huruggamuwa100% (1)
- Phlebotomy and Hematology Exam Review.Documento3 páginasPhlebotomy and Hematology Exam Review.MohamedKeynanAinda não há avaliações
- Specimen CollectionDocumento27 páginasSpecimen CollectionJohny Joseph100% (1)
- Phlebotomy Protocol V4Documento26 páginasPhlebotomy Protocol V4Pedro Pérez100% (1)
- Estimation of Haemoglobin ConcentrationDocumento41 páginasEstimation of Haemoglobin ConcentrationArslan ArshadAinda não há avaliações
- Phlebotomy: Phlebos - Greek Word Meaning "Vein" & Tome - "To Cut"Documento5 páginasPhlebotomy: Phlebos - Greek Word Meaning "Vein" & Tome - "To Cut"Gerald John PazAinda não há avaliações
- Blood Collection TubesDocumento1 páginaBlood Collection TubesMohammad Atiq100% (1)
- Collection of SpecimenDocumento35 páginasCollection of SpecimenRona Palomo100% (1)
- Aubf Lec (2 Week) Physical Examination of Urine: Color, Clarity Specific GravityDocumento38 páginasAubf Lec (2 Week) Physical Examination of Urine: Color, Clarity Specific GravityAngela ReyesAinda não há avaliações
- Medical Laboratory TechnologyDocumento3 páginasMedical Laboratory TechnologyAHMEDAinda não há avaliações
- VenipunctureDocumento13 páginasVenipunctureFatimah Syed OmarAinda não há avaliações
- Sample CollectionDocumento18 páginasSample CollectionAMI KSAAinda não há avaliações
- Chapter OneDocumento53 páginasChapter OnemustangsarahAinda não há avaliações
- Hematocrit and Hemoglobin DeterminationDocumento32 páginasHematocrit and Hemoglobin DeterminationCeliz HilarioAinda não há avaliações
- Phlebotomy Review QuestionsDocumento3 páginasPhlebotomy Review QuestionsMaria Isabel Trujillo ParralesAinda não há avaliações
- Types of Specimen Collection ContainersDocumento7 páginasTypes of Specimen Collection ContainersLucas Dei AmengorAinda não há avaliações
- Policy Phlebotomy Blood CollectionDocumento6 páginasPolicy Phlebotomy Blood CollectionmuhammadhanifmohdfahmiAinda não há avaliações
- Cytology Staining Methods PDFDocumento7 páginasCytology Staining Methods PDFFabrício CamargoAinda não há avaliações
- Phlebotomy Procedure 3rd PDFDocumento4 páginasPhlebotomy Procedure 3rd PDFFranciska Gledy AmbaritaAinda não há avaliações
- Introduction To Blood BankingDocumento65 páginasIntroduction To Blood Bankingpaolo celino100% (1)
- Blood Specimen CollectionDocumento12 páginasBlood Specimen CollectionSamar SharafAinda não há avaliações
- Proper Collection and Preservation of SpecimenDocumento6 páginasProper Collection and Preservation of SpecimenDavid SantosAinda não há avaliações
- Nonblood Specimen CollectionDocumento47 páginasNonblood Specimen CollectionAyeneMarieLugueAinda não há avaliações
- BLOOD TRANSFUSION NotesDocumento7 páginasBLOOD TRANSFUSION NotesErl D. MelitanteAinda não há avaliações
- Plasma ProteinsDocumento11 páginasPlasma ProteinsnirilibAinda não há avaliações
- Stool ExaminationDocumento5 páginasStool ExaminationFrinkaWijayaAinda não há avaliações
- POLYCYTHEMIADocumento48 páginasPOLYCYTHEMIAPoova RagavanAinda não há avaliações
- 01 Blood CollectionDocumento120 páginas01 Blood CollectionBianca OcampoAinda não há avaliações
- Phlebotomy in A NutshellDocumento131 páginasPhlebotomy in A Nutshellgreen_archerAinda não há avaliações
- Blood CollectionDocumento24 páginasBlood CollectionOla ALmadan100% (1)
- Designing A Peace Building InfrastructureDocumento253 páginasDesigning A Peace Building InfrastructureAditya SinghAinda não há avaliações
- Administrator's Guide: SeriesDocumento64 páginasAdministrator's Guide: SeriesSunny SaahilAinda não há avaliações
- Echnical Ocational Ivelihood: Edia and Nformation IteracyDocumento12 páginasEchnical Ocational Ivelihood: Edia and Nformation IteracyKrystelle Marie AnteroAinda não há avaliações
- Framework For Marketing Management Global 6Th Edition Kotler Solutions Manual Full Chapter PDFDocumento33 páginasFramework For Marketing Management Global 6Th Edition Kotler Solutions Manual Full Chapter PDFWilliamThomasbpsg100% (9)
- Chapter 3 - the-WPS OfficeDocumento15 páginasChapter 3 - the-WPS Officekyoshiro RyotaAinda não há avaliações
- Capacitor Banks in Power System Part FourDocumento4 páginasCapacitor Banks in Power System Part FourTigrillo100% (1)
- 1 Mark QuestionsDocumento8 páginas1 Mark QuestionsPhani Chintu100% (2)
- History of Drugs (Autosaved)Documento68 páginasHistory of Drugs (Autosaved)Juan TowTowAinda não há avaliações
- Key Performance IndicatorsDocumento15 páginasKey Performance IndicatorsAbdul HafeezAinda não há avaliações
- 1 - HandBook CBBR4106Documento29 páginas1 - HandBook CBBR4106mkkhusairiAinda não há avaliações
- 67-Article Text-118-1-10-20181206Documento12 páginas67-Article Text-118-1-10-20181206MadelAinda não há avaliações
- An Analysis of The PoemDocumento2 páginasAn Analysis of The PoemDayanand Gowda Kr100% (2)
- Upload A Document To Access Your Download: The Psychology Book, Big Ideas Simply Explained - Nigel Benson PDFDocumento3 páginasUpload A Document To Access Your Download: The Psychology Book, Big Ideas Simply Explained - Nigel Benson PDFchondroc11Ainda não há avaliações
- Effect of Intensive Health Education On Adherence To Treatment in Sputum Positive Pulmonary Tuberculosis PatientsDocumento6 páginasEffect of Intensive Health Education On Adherence To Treatment in Sputum Positive Pulmonary Tuberculosis PatientspocutindahAinda não há avaliações
- Ottley Sandra 2009Documento285 páginasOttley Sandra 2009Lucas Fariña AlheirosAinda não há avaliações
- Trigonometry Primer Problem Set Solns PDFDocumento80 páginasTrigonometry Primer Problem Set Solns PDFderenz30Ainda não há avaliações
- Popular Music Analysis and MusicologyDocumento15 páginasPopular Music Analysis and MusicologyAlexMartínVidal100% (3)
- CopacabanaDocumento2 páginasCopacabanaNereus Sanaani CAñeda Jr.Ainda não há avaliações
- Operational Effectiveness + StrategyDocumento7 páginasOperational Effectiveness + StrategyPaulo GarcezAinda não há avaliações
- Report Body of IIDFC - 2Documento120 páginasReport Body of IIDFC - 2Shanita AhmedAinda não há avaliações
- (U) Daily Activity Report: Marshall DistrictDocumento6 páginas(U) Daily Activity Report: Marshall DistrictFauquier NowAinda não há avaliações
- Ib Physics SL - Unit 4 ReviewDocumento46 páginasIb Physics SL - Unit 4 ReviewMax HudgenesAinda não há avaliações
- Introduction To PTC Windchill PDM Essentials 11.1 For Light UsersDocumento6 páginasIntroduction To PTC Windchill PDM Essentials 11.1 For Light UsersJYAinda não há avaliações
- D8.1M 2007PV PDFDocumento5 páginasD8.1M 2007PV PDFkhadtarpAinda não há avaliações
- EELE 202 Lab 6 AC Nodal and Mesh Analysis s14Documento8 páginasEELE 202 Lab 6 AC Nodal and Mesh Analysis s14Nayr JTAinda não há avaliações
- Grade 3Documento4 páginasGrade 3Shai HusseinAinda não há avaliações
- HRM and The Business EnvironmentDocumento18 páginasHRM and The Business Environmentsuzzette91Ainda não há avaliações
- Ergonomics For The BlindDocumento8 páginasErgonomics For The BlindShruthi PandulaAinda não há avaliações
- Department of Education: Republic of The PhilippinesDocumento2 páginasDepartment of Education: Republic of The PhilippinesShailac RodelasAinda não há avaliações
- MOA Agri BaseDocumento6 páginasMOA Agri BaseRodj Eli Mikael Viernes-IncognitoAinda não há avaliações