Você também pode gostar
- 4-Key Findings From CaprieDocumento30 páginas4-Key Findings From CaprieMuhammad Yolandi SumadioAinda não há avaliações
- CLOPIDOGRELDocumento4 páginasCLOPIDOGRELHuseikha VelayazulfahdAinda não há avaliações
- Acs Slide Utk Ps (Cure) - TranslateDocumento38 páginasAcs Slide Utk Ps (Cure) - TranslateMuhammad Yolandi SumadioAinda não há avaliações
- Journal Club: Presented by - Dr. Harshal Pamecha Resident in Cardiology CMCHDocumento34 páginasJournal Club: Presented by - Dr. Harshal Pamecha Resident in Cardiology CMCHlichumo murryAinda não há avaliações
- ACCP Cardiology PRN JC June 2022Documento16 páginasACCP Cardiology PRN JC June 2022topAinda não há avaliações
- Steroids in Cardiac SurgeryDocumento52 páginasSteroids in Cardiac SurgeryKarthik RamanAinda não há avaliações
- Antiplatelet Agents in Acute Non-ST Elevation Acute Coronary SyndromesDocumento31 páginasAntiplatelet Agents in Acute Non-ST Elevation Acute Coronary SyndromesCésar Santis FuentesAinda não há avaliações
- COMMIT ClopidogrelDocumento15 páginasCOMMIT ClopidogrelCristina PazmiñoAinda não há avaliações
- DR Huma NstemiDocumento114 páginasDR Huma NstemiArzalan BaigAinda não há avaliações
- The Use of Dual Antiplatelet Therapy For Ischemic Cerebrovascular EventsDocumento7 páginasThe Use of Dual Antiplatelet Therapy For Ischemic Cerebrovascular EventsnoiAinda não há avaliações
- CYP450 System and Not BeingDocumento5 páginasCYP450 System and Not BeingArfa'i LaksamanaAinda não há avaliações
- Pegasus TIMI 54 TrialDocumento13 páginasPegasus TIMI 54 TrialIsaac Aaron Enriquez MonsalvoAinda não há avaliações
- High-Dose Clopidogrel, Prasugrel or Ticagrelor: Trying To Unravel A Skein Into A Ball. Alessandro Aprile, Raffaella Marzullo, Giuseppe Biondi Zoccai, Maria Grazia ModenaDocumento8 páginasHigh-Dose Clopidogrel, Prasugrel or Ticagrelor: Trying To Unravel A Skein Into A Ball. Alessandro Aprile, Raffaella Marzullo, Giuseppe Biondi Zoccai, Maria Grazia ModenaDrugs & Therapy StudiesAinda não há avaliações
- AaDocumento9 páginasAatiasabrinaAinda não há avaliações
- Nejmoa 010746Documento9 páginasNejmoa 010746Mmle BlaséAinda não há avaliações
- Cardioprotection by Opening of The K Channel in Unstable AnginaDocumento7 páginasCardioprotection by Opening of The K Channel in Unstable Angina111111111111111111132222Ainda não há avaliações
- Jama You 2020 Oi 200094 1603319690.60891Documento11 páginasJama You 2020 Oi 200094 1603319690.60891edo adimastaAinda não há avaliações
- AntihipertensiDocumento75 páginasAntihipertensimuryaniAinda não há avaliações
- Ticagrelor PDFDocumento7 páginasTicagrelor PDFNurul Masyithah100% (1)
- FluidDocumento190 páginasFluidAndrias OzAinda não há avaliações
- Herbesser StrokeDocumento15 páginasHerbesser StrokePrincess MiraAinda não há avaliações
- 09.30 Professor John Townend, Chest Pain and Troponins On The Acute TakeDocumento39 páginas09.30 Professor John Townend, Chest Pain and Troponins On The Acute Takeamir ahmadAinda não há avaliações
- 19 - 30Documento11 páginas19 - 30Tasya IrwanAinda não há avaliações
- 3745 PDFDocumento6 páginas3745 PDFJanuar RezkyAinda não há avaliações
- White 2012 Champion PooledDocumento13 páginasWhite 2012 Champion PooledRadu CiprianAinda não há avaliações
- 0178959e6a78&ie SdarticleDocumento7 páginas0178959e6a78&ie SdarticleRiza Adi SaputraAinda não há avaliações
- DoneDocumento10 páginasDoneShoaib KhatikAinda não há avaliações
- Stemi Vs NstemiDocumento31 páginasStemi Vs NstemiFadhilAfifAinda não há avaliações
- Nejmc 0909586Documento4 páginasNejmc 0909586theboy14juneAinda não há avaliações
- Beta Blocker in Heart Failure TrailDocumento31 páginasBeta Blocker in Heart Failure Trailgovind rajAinda não há avaliações
- BMJ l2211 Full PDFDocumento11 páginasBMJ l2211 Full PDFdhea handyaraAinda não há avaliações
- Furtado 2016Documento10 páginasFurtado 2016zzzzAinda não há avaliações
- 1 s2.0 S0735109708008656 MainDocumento10 páginas1 s2.0 S0735109708008656 MainraniahAinda não há avaliações
- Jurnal 4 WordDocumento20 páginasJurnal 4 WordSri MaryatiAinda não há avaliações
- MatsutaniDocumento12 páginasMatsutanigarry.soloanAinda não há avaliações
- Evolve Study Journal Club PresentationDocumento62 páginasEvolve Study Journal Club PresentationsantoshvelloreAinda não há avaliações
- BMJ l2211 FullDocumento11 páginasBMJ l2211 FullOeij Henri WijayaAinda não há avaliações
- State of The Art: Critical Conditions: Cardiogenic ShockDocumento30 páginasState of The Art: Critical Conditions: Cardiogenic ShockitsarunachalamAinda não há avaliações
- Joc120067 882 889Documento8 páginasJoc120067 882 889www.manvith8Ainda não há avaliações
- Angina Pectoris Treatment & Management - Medical Care, Surgical Care, PreventionDocumento20 páginasAngina Pectoris Treatment & Management - Medical Care, Surgical Care, Preventionblack_eagel100% (1)
- Dr. Esperanza Cabral ModuleDocumento54 páginasDr. Esperanza Cabral ModuleNazarine TorresAinda não há avaliações
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 2000)Documento56 páginasP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 2000)agaperdana21Ainda não há avaliações
- The Role of CYP2C19 Genotyping To Guide Antiplatelet Therapy Following IschemicDocumento15 páginasThe Role of CYP2C19 Genotyping To Guide Antiplatelet Therapy Following IschemicmedgusAinda não há avaliações
- Dual Antiplatelet Therapy Clopidogrel With Low-Dose Cilostazol Intensifies Platelet Inhibition in Patients With Ischemic StrokeDocumento5 páginasDual Antiplatelet Therapy Clopidogrel With Low-Dose Cilostazol Intensifies Platelet Inhibition in Patients With Ischemic StrokeDhanang Prawira NugrahaAinda não há avaliações
- Eficacia Del Clopidogrel en Pacientes Con Fibrilacion Auricular y Sindrome Coronario AgudoDocumento7 páginasEficacia Del Clopidogrel en Pacientes Con Fibrilacion Auricular y Sindrome Coronario AgudoElva MonserrathAinda não há avaliações
- MinaDocumento6 páginasMinaminamoharebAinda não há avaliações
- Freedom TrialDocumento34 páginasFreedom TrialDaniela DíazAinda não há avaliações
- JNC8 & ChlorthalidoneDocumento69 páginasJNC8 & ChlorthalidoneAkansha KalraAinda não há avaliações
- Safety and Efficacy of Intensive Vs Guideline Antiplatelet Thera 2015Documento7 páginasSafety and Efficacy of Intensive Vs Guideline Antiplatelet Thera 2015AnDreARAinda não há avaliações
- Merec Bulletin Vol15 No6Documento4 páginasMerec Bulletin Vol15 No6n4dn4dAinda não há avaliações
- Terapi Suplementasi Oksigen Pada STEMI 3Documento31 páginasTerapi Suplementasi Oksigen Pada STEMI 3Yeny ElfiyantiAinda não há avaliações
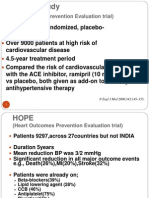
- The HOPE Study: (Heart Outcomes Prevention Evaluation Trial)Documento4 páginasThe HOPE Study: (Heart Outcomes Prevention Evaluation Trial)kurutalaAinda não há avaliações
- Efficacy of Atenolol and Captopril in Reducing Risk of Macrovascular and Microvascular Complications in Type 2 Diabetes: UKPDS 39Documento8 páginasEfficacy of Atenolol and Captopril in Reducing Risk of Macrovascular and Microvascular Complications in Type 2 Diabetes: UKPDS 39Laila MayangsariAinda não há avaliações
- Michele Fang, MD Michele Fang, MD Department of General Department of General Internal Medicine Internal MedicineDocumento30 páginasMichele Fang, MD Michele Fang, MD Department of General Department of General Internal Medicine Internal MedicinemicfangAinda não há avaliações
- Cardiovascular Risk in Clopidogrel-Treated Patients According To Cytochrome P450 2C19 2 Loss-of-Function Allele or Proton Pump Inhibitor CoadministrationDocumento10 páginasCardiovascular Risk in Clopidogrel-Treated Patients According To Cytochrome P450 2C19 2 Loss-of-Function Allele or Proton Pump Inhibitor CoadministrationVenansius ReinaldiAinda não há avaliações
- ASCOT TrialDocumento8 páginasASCOT TrialMigs MedinaAinda não há avaliações
- Fneur 11 00534 PDFDocumento9 páginasFneur 11 00534 PDFOeij Henri WijayaAinda não há avaliações
- Editorial 2Documento4 páginasEditorial 2david1086Ainda não há avaliações
- PLATO糖尿病Documento11 páginasPLATO糖尿病陈诗哲Ainda não há avaliações
- Krebss Home Child Care Consent FormsDocumento2 páginasKrebss Home Child Care Consent FormsAngelaKathleenAinda não há avaliações
- Ingrown Nail RemovalDocumento28 páginasIngrown Nail RemovaljaphetnwapiAinda não há avaliações
- Documentation in Your 3 Year and Beyond: Summer Quarter 2010Documento32 páginasDocumentation in Your 3 Year and Beyond: Summer Quarter 2010Roberto ParedesAinda não há avaliações
- Facilitated Pci Vs Rescue Pci - DR Dolly MathewDocumento51 páginasFacilitated Pci Vs Rescue Pci - DR Dolly MathewJose JacobAinda não há avaliações
- COLONOSCOPY - Details: Study ResultDocumento5 páginasCOLONOSCOPY - Details: Study ResultJaskaran SinghAinda não há avaliações
- Abdominal Trauma - Dr. Febiansyah Ibrahim, SPB-KBDDocumento32 páginasAbdominal Trauma - Dr. Febiansyah Ibrahim, SPB-KBDPrandyAinda não há avaliações
- User Guide For The Participant Use Data File: American College of Surgeons National Surgical Quality Improvement ProgramDocumento40 páginasUser Guide For The Participant Use Data File: American College of Surgeons National Surgical Quality Improvement Programbobobobo12341212Ainda não há avaliações
- VKA in AFDocumento64 páginasVKA in AFบอส เลิศเกียรติรัชตะAinda não há avaliações
- BHD Dan Code Blue PDFDocumento73 páginasBHD Dan Code Blue PDFVira RinandaAinda não há avaliações
- Enhanced Recovery After SurgeryDocumento36 páginasEnhanced Recovery After Surgeryfaundra100% (1)
- LAPAROSCOPIC SURGERyDocumento37 páginasLAPAROSCOPIC SURGERyabraham winartoAinda não há avaliações
- Vivid 3: Cardiovascular Ultrasound SystemDocumento6 páginasVivid 3: Cardiovascular Ultrasound SystemNorthern LightsAinda não há avaliações
- Interpretasi ECG Dr. SallyDocumento66 páginasInterpretasi ECG Dr. SallyRichard GunawanAinda não há avaliações
- Abduraham Rayyan-Module-Cardiovascular-SystemDocumento17 páginasAbduraham Rayyan-Module-Cardiovascular-SystemRAYYAN ENIL ABDURAHAMAinda não há avaliações
- Lesson 5-Chapter 9 Routine VenipunctureDocumento9 páginasLesson 5-Chapter 9 Routine VenipunctureJeffrey FernandezAinda não há avaliações
- DR - Ritty Arouje Recent Question Paper FileDocumento118 páginasDR - Ritty Arouje Recent Question Paper Filemuneer024Ainda não há avaliações
- Gen Pathology CasesDocumento41 páginasGen Pathology Casesrjh18950% (1)
- Club Foot-Dr J SahooDocumento9 páginasClub Foot-Dr J SahooSheel Gupta100% (1)
- Overview of Female Reproductive System ResearchDocumento21 páginasOverview of Female Reproductive System ResearchOmar Ali AyoubkhanAinda não há avaliações
- Mucogingival SurgeryDocumento26 páginasMucogingival SurgeryNathnael GebAinda não há avaliações
- Operative Exam Questions DR Hatem Sahar 2012-2013Documento2 páginasOperative Exam Questions DR Hatem Sahar 2012-2013Abdallah GamalAinda não há avaliações
- Hollow Cheeeks GuideDocumento52 páginasHollow Cheeeks Guidepoomisuk2550Ainda não há avaliações
- Guidelines For Case Classification For The National Birth Defects Prevention StudyDocumento9 páginasGuidelines For Case Classification For The National Birth Defects Prevention Studyjorge davidAinda não há avaliações
- Bone Void Fillers - JAAOS - Journal of The American Academy of Orthopaedic SurgeonsDocumento5 páginasBone Void Fillers - JAAOS - Journal of The American Academy of Orthopaedic SurgeonsmuklisrivaiAinda não há avaliações
- Maryam CV-1 PDFDocumento6 páginasMaryam CV-1 PDFAamir SultanAinda não há avaliações
- Mandible NotesDocumento19 páginasMandible NotescutkarshaAinda não há avaliações
- Surgery 2015 MCQDocumento15 páginasSurgery 2015 MCQMohammad Husni Banisalman83% (6)
- Male and Female Bladder CatheterizationDocumento13 páginasMale and Female Bladder CatheterizationAyen Fornolles100% (1)
- Allomax Surgical Graft Technique GuideDocumento32 páginasAllomax Surgical Graft Technique Guidedr_kumananAinda não há avaliações
- Ecri-Polyurethane 0Documento70 páginasEcri-Polyurethane 0Rami RouhanaAinda não há avaliações