Você também pode gostar
- Reyes, Kay Ma. Pearl Serranilla, Denisa Louise Tan, Francisco III Shivpura Sonia MDocumento50 páginasReyes, Kay Ma. Pearl Serranilla, Denisa Louise Tan, Francisco III Shivpura Sonia MGeraldine Marie Salvo100% (1)
- Biodiversity ActivitiesDocumento11 páginasBiodiversity ActivitiesESMERALDA GAMILAinda não há avaliações
- EpidemiologyDocumento89 páginasEpidemiologyKrishnaveni MurugeshAinda não há avaliações
- 1 - EpidemiologyDocumento26 páginas1 - Epidemiologyhemihema75% (4)
- Uses of EpidemiologyDocumento28 páginasUses of EpidemiologyBinita Shakya0% (1)
- Principles of Epidemiology & Epidemiologic MethodsDocumento62 páginasPrinciples of Epidemiology & Epidemiologic MethodsMonish NavaneethanAinda não há avaliações
- Public Health - Resume of Shah BookDocumento54 páginasPublic Health - Resume of Shah BookKami Dhillon83% (6)
- Epidemiology: RD THDocumento21 páginasEpidemiology: RD THKailash Nagar100% (1)
- Chapter 5 Epidemiology-CphDocumento51 páginasChapter 5 Epidemiology-CphMarcus Randielle FloresAinda não há avaliações
- Energy Pyramaid LabDocumento2 páginasEnergy Pyramaid LabQuinn Jackson100% (1)
- Epidemiology 2Documento54 páginasEpidemiology 2oheneapeahrita100% (2)
- Objectives of EpidemiologyDocumento23 páginasObjectives of EpidemiologyAnitha sujith75% (4)
- EpidemiologyDocumento10 páginasEpidemiologyMUTHUKUMARANAinda não há avaliações
- EpidemiologyDocumento13 páginasEpidemiologyswethashaki50% (2)
- The Study of Disease Distribution and Determinants in PopulationsDocumento39 páginasThe Study of Disease Distribution and Determinants in PopulationsjayalakshmiAinda não há avaliações
- The Concept of Epidemiologic Surveillance: Ari UdijonoDocumento50 páginasThe Concept of Epidemiologic Surveillance: Ari UdijonoariAinda não há avaliações
- Content On EpidemiologyDocumento6 páginasContent On Epidemiologyrakesh rathAinda não há avaliações
- SDG 15: Life On Land: Conserve Terrestrial and Freshwater EcosystemsDocumento25 páginasSDG 15: Life On Land: Conserve Terrestrial and Freshwater EcosystemsShivi AgarwalAinda não há avaliações
- Epidemiology: Dr. Siswanto, M.SCDocumento66 páginasEpidemiology: Dr. Siswanto, M.SCArinTa TyArlieAinda não há avaliações
- EpidemiologyDocumento100 páginasEpidemiologyKailash NagarAinda não há avaliações
- Earth and Life Science Module 198Documento9 páginasEarth and Life Science Module 198Villanueva, MaeAinda não há avaliações
- Chapter 5: Studying Disease DistributionDocumento7 páginasChapter 5: Studying Disease DistributionJohn Rick OrineAinda não há avaliações
- Epidem. Lecture 1 & 2Documento18 páginasEpidem. Lecture 1 & 2sajad abasew100% (1)
- Theories and Models of Disease CausationDocumento62 páginasTheories and Models of Disease CausationsunielgowdaAinda não há avaliações
- Epidemiological MethodsDocumento22 páginasEpidemiological MethodsDolly Dutta0% (1)
- Epidemiology by SamuelDocumento227 páginasEpidemiology by Samueldagimb bekeleAinda não há avaliações
- AMA 4351 Statistical EpidemiologyDocumento72 páginasAMA 4351 Statistical EpidemiologyRobinson WambuaAinda não há avaliações
- "Epidemiology Is The Study of The Distribution and Determinants of Health-The Control of Health ProblemsDocumento11 páginas"Epidemiology Is The Study of The Distribution and Determinants of Health-The Control of Health ProblemsGwen Dennise MisadorAinda não há avaliações
- Definition of EpidemiologyDocumento3 páginasDefinition of EpidemiologyAnneke RamadhantyAinda não há avaliações
- EPIDEMIOLOGY - BevDocumento55 páginasEPIDEMIOLOGY - BevPINAO-AN, ZANNIELLE GEA L.Ainda não há avaliações
- CHN 2Documento13 páginasCHN 2Claire Maurice JuaneroAinda não há avaliações
- Document 4 EPIDEMIOLOGYDocumento14 páginasDocument 4 EPIDEMIOLOGYHardeep KaurAinda não há avaliações
- Epidemiology The Foundation of Public Health PDFDocumento34 páginasEpidemiology The Foundation of Public Health PDFgabe18Ainda não há avaliações
- EpidemiologyDocumento18 páginasEpidemiologyRose Jean C. OtodAinda não há avaliações
- Leading causes of death in the PhilippinesDocumento4 páginasLeading causes of death in the PhilippinesChristian BeneradoAinda não há avaliações
- Distribution and Determinants of DiseaseDocumento6 páginasDistribution and Determinants of DiseaseNoreen FæţįmæAinda não há avaliações
- EpidemiologyDocumento7 páginasEpidemiologyInoxcent MoonAinda não há avaliações
- EPI Lecture1Documento43 páginasEPI Lecture1Margaret SannohAinda não há avaliações
- Epidemiology. Final22Documento11 páginasEpidemiology. Final22Sandhya GuptaAinda não há avaliações
- Lecturenote - 2121234844biostatistics and Epidemiology (Stat3101) Handout Chapter-1Documento20 páginasLecturenote - 2121234844biostatistics and Epidemiology (Stat3101) Handout Chapter-1McLord SelasiAinda não há avaliações
- 1 Introduction To EpidemiologyDocumento2 páginas1 Introduction To EpidemiologymonishaAinda não há avaliações
- Epidemiological Research ExplainedDocumento2 páginasEpidemiological Research ExplainedKashyAinda não há avaliações
- 1 Epidemiology DefinicaoemarcoshistoricosDocumento19 páginas1 Epidemiology DefinicaoemarcoshistoricosHelioPassulequeAinda não há avaliações
- Topic 1 A Public Health ApproachDocumento5 páginasTopic 1 A Public Health ApproachAldren BeliberAinda não há avaliações
- محاضرة الرابعة اختياريةDocumento8 páginasمحاضرة الرابعة اختياريةGossoon ElywyAinda não há avaliações
- LI LBM 1 Modul SKNDocumento12 páginasLI LBM 1 Modul SKNzashenaAinda não há avaliações
- Role of The Public Health NurseDocumento8 páginasRole of The Public Health NurseRaynelah AnnAinda não há avaliações
- Study DesignDocumento3 páginasStudy Designmusa onyango obuyaAinda não há avaliações
- Lect 1 EgidemiologyDocumento25 páginasLect 1 EgidemiologyMai MaiAinda não há avaliações
- EPI Lecture Note April 2005, YemaneDocumento132 páginasEPI Lecture Note April 2005, YemaneGetahun TekleAinda não há avaliações
- 1introduction To EpidemiologyDocumento10 páginas1introduction To EpidemiologyalhashemisaqrAinda não há avaliações
- Epidemiology Is The Study of Patterns ofDocumento5 páginasEpidemiology Is The Study of Patterns oflawbondAinda não há avaliações
- Jurnal KedokteranDocumento18 páginasJurnal KedokteranelvandryAinda não há avaliações
- Definition and Aim of EpidemiologyDocumento25 páginasDefinition and Aim of EpidemiologyJeevan KumarAinda não há avaliações
- 2) Public Health and EpidemiologyDocumento34 páginas2) Public Health and EpidemiologyDr. Zirwa AsimAinda não há avaliações
- 500-Word Essay: Epidemiological StudiesDocumento4 páginas500-Word Essay: Epidemiological StudiesmuhdfarhanAinda não há avaliações
- Epidemiology: The Study of Disease DistributionDocumento3 páginasEpidemiology: The Study of Disease Distributionغدير ميثاق شمخي جبرAinda não há avaliações
- Epidemiology - Intro - 11Documento58 páginasEpidemiology - Intro - 11Tin WannAinda não há avaliações
- Introduction To Epidemiology 22.09.2021Documento30 páginasIntroduction To Epidemiology 22.09.2021Valdez CavadimaAinda não há avaliações
- Epidemiology NewDocumento26 páginasEpidemiology NewBabita DhruwAinda não há avaliações
- Principles of EpidemiologyDocumento5 páginasPrinciples of EpidemiologyJaffar ZabertAinda não há avaliações
- Epi Lecture 1 Part IIDocumento36 páginasEpi Lecture 1 Part IIMowlidAbdirahman Ali madaaleAinda não há avaliações
- EpidemiologyDocumento36 páginasEpidemiologyhendra2darmawan50% (2)
- Rate Adjustment ExerciseDocumento6 páginasRate Adjustment ExercisemelavinAinda não há avaliações
- FIELD TRIP MuthamakiDocumento10 páginasFIELD TRIP MuthamakimelavinAinda não há avaliações
- Mental HealthDocumento2 páginasMental HealthmelavinAinda não há avaliações
- Field Attachment Report at Chuka HospitalDocumento21 páginasField Attachment Report at Chuka Hospitalmelavin100% (1)
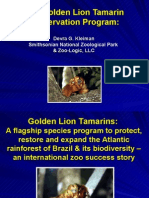
- The Golden Lion Tamarin Conservation ProgramDocumento37 páginasThe Golden Lion Tamarin Conservation ProgramEnvironmental Evaluators NetworkAinda não há avaliações
- Environmental Changes and Challenges of Tarai and Siwalik of NepalDocumento323 páginasEnvironmental Changes and Challenges of Tarai and Siwalik of NepalManika ManikaAinda não há avaliações
- Nature 'S Guardian Nature 'S GuardianDocumento10 páginasNature 'S Guardian Nature 'S GuardianIshika LuckhunAinda não há avaliações
- Energy Flow Through The EcosystemDocumento5 páginasEnergy Flow Through The EcosystemCiprian BitcaAinda não há avaliações
- Kecenderungan Ars Abad 21Documento21 páginasKecenderungan Ars Abad 21fadlifaozyAinda não há avaliações
- Sustainabilityinbuilding PDFDocumento9 páginasSustainabilityinbuilding PDFTaanayaAinda não há avaliações
- Oslo Statement On Ecotourism - August 2007 (English)Documento8 páginasOslo Statement On Ecotourism - August 2007 (English)The International Ecotourism SocietyAinda não há avaliações
- Message From Ms Audrey Azoulay, Director-General of UNESCO, On The Occasion of World Environment Day - Beat Plastic PollutionDocumento2 páginasMessage From Ms Audrey Azoulay, Director-General of UNESCO, On The Occasion of World Environment Day - Beat Plastic PollutionZheng WUAinda não há avaliações
- ENVM 8006A Lecture 1A-Introduction (2022-23)Documento43 páginasENVM 8006A Lecture 1A-Introduction (2022-23)sadgsgAinda não há avaliações
- Themes For DiscussionDocumento24 páginasThemes For DiscussionRavenal Dela FuenteAinda não há avaliações
- 5 Ways to Conserve Biodiversity and Protect EcosystemsDocumento14 páginas5 Ways to Conserve Biodiversity and Protect Ecosystemsjackie varquezAinda não há avaliações
- Luas Minimum dan Metode Kuadrat untuk Analisis VegetasiDocumento11 páginasLuas Minimum dan Metode Kuadrat untuk Analisis VegetasiNabila AzraAinda não há avaliações
- ScorecardDocumento1 páginaScorecardYves NkamgniaAinda não há avaliações
- .3is - LESSON PLANDocumento9 páginas.3is - LESSON PLANMary Ann SuanAinda não há avaliações
- Dan Jared E. Origines BSA-2 Laudato Si': Reflection PaperDocumento1 páginaDan Jared E. Origines BSA-2 Laudato Si': Reflection PaperMarie Sheryl FernandezAinda não há avaliações
- 7th Science Calamity 2Documento12 páginas7th Science Calamity 2yasser yousriAinda não há avaliações
- 12.0 Ecosystem Ecology Recap: 12.1 Energy Flow and Chemical CyclingDocumento5 páginas12.0 Ecosystem Ecology Recap: 12.1 Energy Flow and Chemical CyclingOtiosse MyosotisAinda não há avaliações
- Understanding Natural ResourcesDocumento4 páginasUnderstanding Natural ResourcessandeepAinda não há avaliações
- Chapter 4 Population EcologyDocumento29 páginasChapter 4 Population EcologyRobin Tobar100% (1)
- Program (ASL) Is A Regional Initiative Where BrazilDocumento7 páginasProgram (ASL) Is A Regional Initiative Where Brazilfajar_k2001Ainda não há avaliações
- Suiza InformacionDocumento1 páginaSuiza InformacionZoraida Ortega PoloAinda não há avaliações
- G7 EcosystemDocumento12 páginasG7 EcosystemPersonalAinda não há avaliações
- Assessment of Ethiopian Sustainable Development Through Green Building ConstructionDocumento12 páginasAssessment of Ethiopian Sustainable Development Through Green Building ConstructionDomach Keak Rom100% (3)
- Lesson 4 Reporter (Villanueva, Singson, Belarmino)Documento55 páginasLesson 4 Reporter (Villanueva, Singson, Belarmino)Kirby ZaragozaAinda não há avaliações
- Human Ecology ReviewDocumento180 páginasHuman Ecology ReviewtaoufikAinda não há avaliações
- Alex O. Awiti BioDocumento1 páginaAlex O. Awiti BioAlex AwitiAinda não há avaliações