Você também pode gostar
- Topnotch Lab Interpretation For MoonlightersDocumento41 páginasTopnotch Lab Interpretation For Moonlightersmefav7778520Ainda não há avaliações
- 5.nephritic SyndromeDocumento64 páginas5.nephritic Syndromeyeni100% (1)
- Urine AnalysisDocumento43 páginasUrine AnalysisBayan MahmoudAinda não há avaliações
- Baza III Curs MedDocumento117 páginasBaza III Curs MedIntekhabAtahar0% (1)
- Child With HematuriaDocumento42 páginasChild With HematuriaalaaAinda não há avaliações
- Pediatric Hematuria Guide: Causes, Evaluation and ManagementDocumento40 páginasPediatric Hematuria Guide: Causes, Evaluation and ManagementAnoop ThoombayilAinda não há avaliações
- HematuriaDocumento14 páginasHematuriahamidAinda não há avaliações
- HematuriaDocumento42 páginasHematuriaWasim R. IssaAinda não há avaliações
- Hematuria in ChildrenDocumento27 páginasHematuria in ChildrenKousik AmancharlaAinda não há avaliações
- HematuriaDocumento51 páginasHematuriaRam ManoharAinda não há avaliações
- Urinary Symptoms - DR RashaDocumento70 páginasUrinary Symptoms - DR RashaRasha TelebAinda não há avaliações
- Causes, Types and Evaluation of HematuriaDocumento34 páginasCauses, Types and Evaluation of HematuriaSai RakshikaAinda não há avaliações
- HematuriaDocumento42 páginasHematuriaAhmad SobihAinda não há avaliações
- Dr. YeshwiniDocumento34 páginasDr. YeshwiniSai RakshikaAinda não há avaliações
- Henoch Schonlein Purpura: Dr. Hendratno Halim, Sp. ADocumento29 páginasHenoch Schonlein Purpura: Dr. Hendratno Halim, Sp. AYulius Eka Agung Seputra, MSiAinda não há avaliações
- Laboratory Interpretation Made Easy: Diana Tamondong-Lachica, MD, FPCPDocumento41 páginasLaboratory Interpretation Made Easy: Diana Tamondong-Lachica, MD, FPCPmarieAinda não há avaliações
- Cerebrospinal Fluid: Gonzalo B. Roman JR.,MD.,FPSPDocumento19 páginasCerebrospinal Fluid: Gonzalo B. Roman JR.,MD.,FPSPBenjamin PrabhuAinda não há avaliações
- Red Urine: Approach To Hematuria in ChildrenDocumento26 páginasRed Urine: Approach To Hematuria in ChildrenGhaithAinda não há avaliações
- Hematuri IPD 2014Documento36 páginasHematuri IPD 2014arlan_nasution05Ainda não há avaliações
- 22 - Proteinuria and HematuriaDocumento73 páginas22 - Proteinuria and HematuriaArsalan NadeemAinda não há avaliações
- OUM Tutorial 1 SBNS3504 RenalDocumento51 páginasOUM Tutorial 1 SBNS3504 RenalMashanimy HoneyAinda não há avaliações
- Microscopic Hematuria-How To ApproachDocumento16 páginasMicroscopic Hematuria-How To ApproachMagesh VaiyapuriAinda não há avaliações
- L1 - Symptoms of UtDocumento55 páginasL1 - Symptoms of UtAhmad SobihAinda não há avaliações
- Toronto Notes Nephrology 2015 21Documento1 páginaToronto Notes Nephrology 2015 21JUSASBAinda não há avaliações
- Differential Diagnosis HematuriaDocumento12 páginasDifferential Diagnosis HematuriairmaAinda não há avaliações
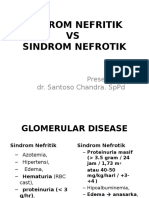
- Nephrotic Syndrome Vs Nephritic SyndromeDocumento46 páginasNephrotic Syndrome Vs Nephritic SyndromelilisAinda não há avaliações
- Approach To Hematuria and Proteinuria in ChildrenDocumento52 páginasApproach To Hematuria and Proteinuria in ChildrenMysheb SS100% (1)
- Glomerular Diseases and The Nephrotic SyndromeDocumento67 páginasGlomerular Diseases and The Nephrotic SyndromeMatyie SmkasAinda não há avaliações
- Sindroma Nefrotik Vs NefritikDocumento23 páginasSindroma Nefrotik Vs NefritikBetha456100% (1)
- Approach To Patient With Renal DiseaseDocumento74 páginasApproach To Patient With Renal DiseaseSaja SaqerAinda não há avaliações
- Sindroma Nefrotik Vs NefritikDocumento23 páginasSindroma Nefrotik Vs NefritikUswatun Aortatika KhasanahAinda não há avaliações
- Case 2Documento4 páginasCase 2Kim Ruiz100% (1)
- Nephrotic and Nephritic Syndrome: Med5010 LectureDocumento65 páginasNephrotic and Nephritic Syndrome: Med5010 LectureFreeburn Simunchembu100% (1)
- Sindroma Nefrotik Vs NefritikDocumento23 páginasSindroma Nefrotik Vs NefritiksiayuAinda não há avaliações
- Renal ProblemsDocumento23 páginasRenal ProblemsMuhammad MakkiAinda não há avaliações
- Describe The Differential Diagnosis of The Common Causes of Hematuria Based On Either Etiological or Anatomic ConsiderationsDocumento13 páginasDescribe The Differential Diagnosis of The Common Causes of Hematuria Based On Either Etiological or Anatomic ConsiderationsNathan JeffreyAinda não há avaliações
- Acute Post-Streptococcal GlomerulonephritisDocumento27 páginasAcute Post-Streptococcal GlomerulonephritisAlokh Saha RajAinda não há avaliações
- Clinical Features of Renal DiseaseDocumento80 páginasClinical Features of Renal DiseaseIdiAmadouAinda não há avaliações
- Case of Obstructive JaundiceDocumento38 páginasCase of Obstructive JaundiceJay R Plogio100% (2)
- UPPER GASTROINTESTINAL BLEEDING (UGIB) MANAGEMENTDocumento47 páginasUPPER GASTROINTESTINAL BLEEDING (UGIB) MANAGEMENTcopperAinda não há avaliações
- Figure 61-2 Approach To The Patient With HematuriaDocumento3 páginasFigure 61-2 Approach To The Patient With HematuriaGood Luck sumsAinda não há avaliações
- CKDDocumento48 páginasCKDJuniorAinda não há avaliações
- Acute Urinary Retention & Hematuria: DR - NOURA Alshahrani Pgy1, Sbem at AchDocumento22 páginasAcute Urinary Retention & Hematuria: DR - NOURA Alshahrani Pgy1, Sbem at AchSalman AlawashizAinda não há avaliações
- Glomerular Disorders - Part I & Part II (ARI NOTES)Documento144 páginasGlomerular Disorders - Part I & Part II (ARI NOTES)Laiba FatimaAinda não há avaliações
- Approach To A Child With HematuriaDocumento13 páginasApproach To A Child With HematuriaSaadAinda não há avaliações
- Nephritic, Nephrotic Syndrome and Acute Kidney Injury in ChildrenDocumento79 páginasNephritic, Nephrotic Syndrome and Acute Kidney Injury in ChildrenB AuAinda não há avaliações
- Approach To HematuriaDocumento45 páginasApproach To HematuriaArun GeorgeAinda não há avaliações
- Glomerulonefrita Acuta Poststreptococica (GNAPS) - Engleza 2 (User-PC - S Conflicted Copy 2013-04-29) - 1Documento37 páginasGlomerulonefrita Acuta Poststreptococica (GNAPS) - Engleza 2 (User-PC - S Conflicted Copy 2013-04-29) - 1Ashley PaulAinda não há avaliações
- Nephrotic Syndrome: By: Yeni Ayu Prihastuti Moderator: DR. Dr. Hani Susianti, SP - PK (K)Documento42 páginasNephrotic Syndrome: By: Yeni Ayu Prihastuti Moderator: DR. Dr. Hani Susianti, SP - PK (K)yeniAinda não há avaliações
- Change in Urine Color (2Documento38 páginasChange in Urine Color (2Mustafa LaithAinda não há avaliações
- Routine Examination of Urine AND It'S InterpretationDocumento64 páginasRoutine Examination of Urine AND It'S InterpretationmeherulafmcAinda não há avaliações
- Sindroma Nefrotik Vs NefritikDocumento23 páginasSindroma Nefrotik Vs NefritikBobby Fildian Siswanto100% (3)
- Urine Dipstick Testing + Common Renal Problem 2012Documento52 páginasUrine Dipstick Testing + Common Renal Problem 2012Ainul ArinaAinda não há avaliações
- 01 Renal System NotesDocumento22 páginas01 Renal System NotesLexanCantorFermoAinda não há avaliações
- Approach To A Child With Hematuria:: Sunil Agrawal 1 Year MD Pediatrics, IOMDocumento42 páginasApproach To A Child With Hematuria:: Sunil Agrawal 1 Year MD Pediatrics, IOMAnthony Salazar RodríguezAinda não há avaliações
- Inflammatory Pelvic DiseaseDocumento17 páginasInflammatory Pelvic DiseaseAnthony Salazar RodríguezAinda não há avaliações
- IDSA Guidelines for Treating MRSA InfectionsDocumento38 páginasIDSA Guidelines for Treating MRSA InfectionsAnthony Salazar RodríguezAinda não há avaliações
- Antidesmoglein 3Documento5 páginasAntidesmoglein 3Anthony Salazar RodríguezAinda não há avaliações
- Highlights of The 2010 American Heart AssociationDocumento1 páginaHighlights of The 2010 American Heart AssociationAnthony Salazar RodríguezAinda não há avaliações
- Factors That Predict Poor Clinical Course Among Patients Hospitalized With Pelvic Inflammatory DiseaseDocumento6 páginasFactors That Predict Poor Clinical Course Among Patients Hospitalized With Pelvic Inflammatory DiseaseAnthony Salazar RodríguezAinda não há avaliações
- Nejmoa1312173 AppendixDocumento14 páginasNejmoa1312173 AppendixAnthony Salazar RodríguezAinda não há avaliações
- Peptic Ulcer Disease: Kalyanakrishnan Ramakrishnan, MD, Frcse, and Robert C. Salinas, MDDocumento8 páginasPeptic Ulcer Disease: Kalyanakrishnan Ramakrishnan, MD, Frcse, and Robert C. Salinas, MDMonika WerdiningsihAinda não há avaliações
- Summit 2 WB Unit 5Documento12 páginasSummit 2 WB Unit 5Anthony Salazar RodríguezAinda não há avaliações
- Crit Drugs TinyDocumento1 páginaCrit Drugs TinyAnthony Salazar RodríguezAinda não há avaliações
- Scalable NetworkingDocumento79 páginasScalable NetworkingAnthony Salazar RodríguezAinda não há avaliações
- Ob AssessmentDocumento7 páginasOb AssessmentAlyssa LippAinda não há avaliações
- Breast Diseases: Assistant Professor Dr. Hiwa Omer AhmedDocumento28 páginasBreast Diseases: Assistant Professor Dr. Hiwa Omer Ahmeddrhiwaomer100% (1)
- NaproxenDocumento3 páginasNaproxenapi-3797941Ainda não há avaliações
- Reading Test 1 Part A Time Limit and InstructionsDocumento9 páginasReading Test 1 Part A Time Limit and Instructionsmathews v.vAinda não há avaliações
- NCFL - 2007 05 16Documento65 páginasNCFL - 2007 05 16Tim RikerAinda não há avaliações
- Test 1 Science Form 3Documento7 páginasTest 1 Science Form 3Zunaizah Yahaya100% (1)
- Addendum To Cover LetterDocumento2 páginasAddendum To Cover LettergfghfAinda não há avaliações
- VegetarianismDocumento3 páginasVegetarianismRadha K dasAinda não há avaliações
- Pott's Disease Night SweatsDocumento22 páginasPott's Disease Night SweatsjesuitkrisAinda não há avaliações
- Is Your Child Doctor or Engineer? - : Combinations For Medical ProfessionDocumento4 páginasIs Your Child Doctor or Engineer? - : Combinations For Medical ProfessionjanakrajchauhanAinda não há avaliações
- Approach To Anaemia: Sameh S El-Atawy 2009Documento37 páginasApproach To Anaemia: Sameh S El-Atawy 2009Sameh Samir El-AtawyAinda não há avaliações
- Vijay D. Wagh - 2013Documento12 páginasVijay D. Wagh - 2013AlyaefkageAinda não há avaliações
- UrethritisDocumento11 páginasUrethritisgreggy_rebel17Ainda não há avaliações
- Total Abdominal Hysterectomy GuideDocumento8 páginasTotal Abdominal Hysterectomy GuidenidoAinda não há avaliações
- What Is Lichen Planus?Documento8 páginasWhat Is Lichen Planus?Asharib AfsarAinda não há avaliações
- C-Reactive Protein Test Details for Inflammation and InfectionDocumento2 páginasC-Reactive Protein Test Details for Inflammation and InfectionPorcha PacsayAinda não há avaliações
- Fluids P GNTDocumento32 páginasFluids P GNTJacinth Florido FedelinAinda não há avaliações
- CARE Newsletter - July 2012Documento12 páginasCARE Newsletter - July 2012Mike RalstonAinda não há avaliações
- Miso Soup For GERDDocumento7 páginasMiso Soup For GERDRippie RifdahAinda não há avaliações
- Top 10 Calcium Rich FoodsDocumento5 páginasTop 10 Calcium Rich Foodsjohn briAinda não há avaliações
- Fosamax Plus FinalDocumento5 páginasFosamax Plus FinalRobin LimAinda não há avaliações
- Management of Diabetic KetoacidosisDocumento23 páginasManagement of Diabetic KetoacidosisAjay DherwaniAinda não há avaliações
- J.P. Morgan Healthcare Conference Chair Discusses AbbVie GrowthDocumento20 páginasJ.P. Morgan Healthcare Conference Chair Discusses AbbVie Growth123456789Ainda não há avaliações
- EndometriomaDocumento7 páginasEndometriomaErick Rafael AncaAinda não há avaliações
- Respiratory Step 2 CK NoteDocumento41 páginasRespiratory Step 2 CK NoteXboyx MahdiAinda não há avaliações
- Jurnal Hafis Fix TampilDocumento14 páginasJurnal Hafis Fix TampilAnonymous Skzf3D2HAinda não há avaliações
- Granuloma Inguinale 2Documento32 páginasGranuloma Inguinale 2Elsa MayoraAinda não há avaliações
- Final NegotiationDocumento4 páginasFinal NegotiationAafreenAinda não há avaliações
- Everything You Need to Get StartedDocumento55 páginasEverything You Need to Get StarteduserAinda não há avaliações