Você também pode gostar
- Data Thermal Printer CSDocumento24 páginasData Thermal Printer CSDedy Chandra HariyonoAinda não há avaliações
- KlikBCA Individual Save PageDocumento1 páginaKlikBCA Individual Save PageDedy Chandra HariyonoAinda não há avaliações
- Manufacturing and ServicesDocumento1 páginaManufacturing and ServicesDedy Chandra HariyonoAinda não há avaliações
- Promoting Products: Brand of Product Product Category Company ShapeDocumento2 páginasPromoting Products: Brand of Product Product Category Company ShapeDedy Chandra HariyonoAinda não há avaliações
- CV (Yessy)Documento1 páginaCV (Yessy)Dedy Chandra HariyonoAinda não há avaliações
- Manufacturing and ServicesDocumento1 páginaManufacturing and ServicesDedy Chandra HariyonoAinda não há avaliações
- CV (Yessy)Documento1 páginaCV (Yessy)Dedy Chandra HariyonoAinda não há avaliações
- Manufacturing and ServicesDocumento1 páginaManufacturing and ServicesDedy Chandra HariyonoAinda não há avaliações
- ManagementDocumento1 páginaManagementDedy Chandra HariyonoAinda não há avaliações
- Promoting Products: Brand of Product Product Category Company ShapeDocumento2 páginasPromoting Products: Brand of Product Product Category Company ShapeDedy Chandra HariyonoAinda não há avaliações
- KlikBCA Individual Save Page - JPGGDocumento1 páginaKlikBCA Individual Save Page - JPGGDedy Chandra HariyonoAinda não há avaliações
- CV (Yessy)Documento1 páginaCV (Yessy)Dedy Chandra HariyonoAinda não há avaliações
- Figo SteroidDocumento14 páginasFigo SteroidDedy Chandra HariyonoAinda não há avaliações
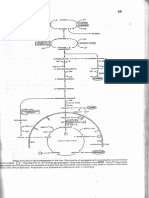
- Glukoneogenesis (Dr. Hairrudin)Documento1 páginaGlukoneogenesis (Dr. Hairrudin)devezzfilAinda não há avaliações
- Pericarditis and Pericardial EffusionDocumento31 páginasPericarditis and Pericardial EffusionDedy Chandra HariyonoAinda não há avaliações
- Insya AllahDocumento1 páginaInsya AllahDedy Chandra HariyonoAinda não há avaliações
- 1015Documento7 páginas1015Bang DeAinda não há avaliações
- TorrentDocumento1 páginaTorrentDedy Chandra HariyonoAinda não há avaliações
- Herbalife 1 - Slimming at All Costs: HerbalifeÒ-induced Liver InjuryDocumento3 páginasHerbalife 1 - Slimming at All Costs: HerbalifeÒ-induced Liver InjuryMohammed AyubAinda não há avaliações
- Makanan PengawetDocumento6 páginasMakanan PengawetDedy Chandra HariyonoAinda não há avaliações
- TorrentDocumento1 páginaTorrentDedy Chandra HariyonoAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Navel DisplacementDocumento4 páginasNavel Displacementdinesh100% (1)
- Flexi Medical Plan BrochureDocumento28 páginasFlexi Medical Plan BrochurewoodksdAinda não há avaliações
- Yoga Therapy For Simple Back PainDocumento7 páginasYoga Therapy For Simple Back Painpartheeban25Ainda não há avaliações
- Acute Rheumatic FeverDocumento9 páginasAcute Rheumatic FeverHarish Kumar KumawatAinda não há avaliações
- Professional ResumeDocumento3 páginasProfessional ResumeUc OhiriAinda não há avaliações
- Pathophysiology: United StatesDocumento11 páginasPathophysiology: United StatesNurullia RahmawatiAinda não há avaliações
- Marsupialization Enucleation in Treatment of Cysts of Oral Cavity Oral SurgeryDocumento22 páginasMarsupialization Enucleation in Treatment of Cysts of Oral Cavity Oral SurgeryFourthMolar.com100% (1)
- ST UWH I 16Documento146 páginasST UWH I 16Lina Ramadhani Anan AsrawiAinda não há avaliações
- Improving pain outcomes for children in surgeryDocumento89 páginasImproving pain outcomes for children in surgeryahmeddammAinda não há avaliações
- Juvenile DelinquencyDocumento43 páginasJuvenile DelinquencyDonnie Ray Olivarez Solon100% (3)
- New Titles from CBS Publishers & DistributorsDocumento24 páginasNew Titles from CBS Publishers & DistributorsBhavya PatelAinda não há avaliações
- Nature's Healing Powers: A Mind-Body Wellness ModelDocumento9 páginasNature's Healing Powers: A Mind-Body Wellness ModelOlivier BenarrocheAinda não há avaliações
- CH14:Managing: A Competency Based Approach, Hellriegel & JacksonDocumento35 páginasCH14:Managing: A Competency Based Approach, Hellriegel & Jacksonsweetyraj100% (2)
- 746259ku PDFDocumento13 páginas746259ku PDFTinkuAinda não há avaliações
- Nutritional Management of Chyle Leaks: An Update: Nutrition Issues in Gastroenterology, Series #94Documento13 páginasNutritional Management of Chyle Leaks: An Update: Nutrition Issues in Gastroenterology, Series #94mmmdeandradeAinda não há avaliações
- 98 PAGE Sample Office Policy and ProceduresDocumento98 páginas98 PAGE Sample Office Policy and ProceduresDenise MathreAinda não há avaliações
- Terapia Clark Biofeedback ZapperDocumento8 páginasTerapia Clark Biofeedback ZapperGomez Gomez50% (2)
- Motor Control Theories: Presented By: PETETI SAIRAM MPT 2 YearDocumento28 páginasMotor Control Theories: Presented By: PETETI SAIRAM MPT 2 YearSai RamAinda não há avaliações
- Medical PluralismDocumento29 páginasMedical PluralismGian pagadduAinda não há avaliações
- Live Your Dreams.Documento2 páginasLive Your Dreams.dholed100% (1)
- NCP FormatDocumento3 páginasNCP FormatAl Bhert Timbal MagbalotAinda não há avaliações
- Human Kinetics: 2019 Product GuideDocumento48 páginasHuman Kinetics: 2019 Product GuideJuanma GonzalezAinda não há avaliações
- Antidote List 2 2011 PDFDocumento12 páginasAntidote List 2 2011 PDFRiZqi RufiAinda não há avaliações
- CMR June LizaDocumento39 páginasCMR June LizaRio PortoAinda não há avaliações
- Penyesuaian Dosis Regimen Pada Pasien Dengan Gangguan Fungsi GinjalDocumento19 páginasPenyesuaian Dosis Regimen Pada Pasien Dengan Gangguan Fungsi GinjalChamidRiyadiAinda não há avaliações
- What Is Delusional Disorder?Documento2 páginasWhat Is Delusional Disorder?Rizki Muhammad RanandaAinda não há avaliações
- 079 BorseDocumento9 páginas079 BorsepuriwatiAinda não há avaliações
- Adrenal Gland DisordersDocumento7 páginasAdrenal Gland Disorderscn351073Ainda não há avaliações
- Access To Special Care Dentistry, Part 5. Safety: A. Dougall and J. FiskeDocumento14 páginasAccess To Special Care Dentistry, Part 5. Safety: A. Dougall and J. FiskeMostafa FayadAinda não há avaliações