Você também pode gostar
- GCT For Dummies - Publish AbleDocumento24 páginasGCT For Dummies - Publish AblepcrosleyAinda não há avaliações
- RCOG Cardiac Disease and Pregnancy PDFDocumento18 páginasRCOG Cardiac Disease and Pregnancy PDFSteven SetioAinda não há avaliações
- Physiologic Changes During Pregnancy and DeliveryDocumento13 páginasPhysiologic Changes During Pregnancy and DeliveryBudi Khang100% (1)
- Iron MetabolismDocumento21 páginasIron MetabolismInês FerreiraAinda não há avaliações
- Post Partum Haem.Documento90 páginasPost Partum Haem.rachael annorAinda não há avaliações
- Cardiac Disease in PregnancyDocumento28 páginasCardiac Disease in PregnancyviharadewiAinda não há avaliações
- Hypertension and Angina DrugsDocumento158 páginasHypertension and Angina DrugsMelissa SalayogAinda não há avaliações
- MANAGEMENT OF EPILEPSY IN PREGNANCYDocumento24 páginasMANAGEMENT OF EPILEPSY IN PREGNANCYClaudio UdjajaAinda não há avaliações
- Sepsis Management PDFDocumento118 páginasSepsis Management PDFsarita julia putriAinda não há avaliações
- Antiphospholipid Syndrome in Pregnancy: Review of Diagnosis and TreatmentDocumento7 páginasAntiphospholipid Syndrome in Pregnancy: Review of Diagnosis and TreatmentDara Dasawulansari SyamsuriAinda não há avaliações
- Fetal Growth Restriction - ACOG 2019Documento23 páginasFetal Growth Restriction - ACOG 2019Adhitya Yudha MaulanaAinda não há avaliações
- Massive Blood Transfusion by DR - BhanumurthyDocumento26 páginasMassive Blood Transfusion by DR - BhanumurthyPrakash Theegela Surya NagaAinda não há avaliações
- Obstetric Summm 1Documento46 páginasObstetric Summm 1ملك عيسىAinda não há avaliações
- Normal Puerperium: Dr. Neetu Singh Sulemani BHMS, MD (Hom) Professor HOD Deptt Obs & Gyn Mnhmc&Ri BikanerDocumento31 páginasNormal Puerperium: Dr. Neetu Singh Sulemani BHMS, MD (Hom) Professor HOD Deptt Obs & Gyn Mnhmc&Ri BikanerYamini Soni100% (1)
- Heart Disease Complicating PregnancyDocumento169 páginasHeart Disease Complicating PregnancyRajeev Sood100% (2)
- Obstetric Anal Sphincter Injury (OASIS) - UpToDateDocumento39 páginasObstetric Anal Sphincter Injury (OASIS) - UpToDateErickAinda não há avaliações
- Post Antibiotic Era Emerging Concern To HumanityDocumento47 páginasPost Antibiotic Era Emerging Concern To Humanitytummalapalli venkateswara raoAinda não há avaliações
- Shoulder Dystocia 1Documento38 páginasShoulder Dystocia 1emilynorchidAinda não há avaliações
- Neonatal JaundiceDocumento72 páginasNeonatal JaundiceThya HakimAinda não há avaliações
- Hemorrhagic Disease of Newborn PDFDocumento2 páginasHemorrhagic Disease of Newborn PDFIndah Paradifa SariAinda não há avaliações
- First Trimester BleedingDocumento12 páginasFirst Trimester BleedingKevin de SilvaAinda não há avaliações
- Spontaneous Delivery in Post-Term PregnancyDocumento55 páginasSpontaneous Delivery in Post-Term Pregnancyr.pavinvikneshAinda não há avaliações
- Antibiotic Use in Critical Care: DR Radha Sundaram Lead Clinician RAH PaisleyDocumento36 páginasAntibiotic Use in Critical Care: DR Radha Sundaram Lead Clinician RAH PaisleyHidayati IdaAinda não há avaliações
- Endometrial Cancer ESMO Clinical Practice GuidelinesDocumento5 páginasEndometrial Cancer ESMO Clinical Practice Guidelinesjhon heriansyahAinda não há avaliações
- Neurological Deseases in PregnancyDocumento6 páginasNeurological Deseases in PregnancyOdi KaiAinda não há avaliações
- Birth History-Feeding PediaDocumento2 páginasBirth History-Feeding Pediachocoholic potchiAinda não há avaliações
- Cardiac Disease in PregnancyDocumento44 páginasCardiac Disease in PregnancyNariska Cooper100% (1)
- Regulation of Iron MetabolismDocumento21 páginasRegulation of Iron MetabolismElita Maritan SAinda não há avaliações
- Fibroids: 1. Red DegenerationDocumento2 páginasFibroids: 1. Red Degenerationcgao30Ainda não há avaliações
- Arrest of DescentDocumento24 páginasArrest of DescentGunawan Efri SAinda não há avaliações
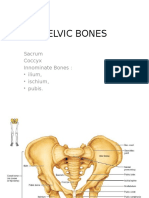
- Pelvic BoneDocumento15 páginasPelvic BoneYoanneveline TanakAinda não há avaliações
- OB - CPG HTN in Pregnancy BEADocumento138 páginasOB - CPG HTN in Pregnancy BEAEllieAdlerAinda não há avaliações
- Disseminated Intravascular Coagulation: Keith Lewis, MDDocumento37 páginasDisseminated Intravascular Coagulation: Keith Lewis, MDRitamaria100% (1)
- Neonatal Hyperbilirubinemia ManagementDocumento76 páginasNeonatal Hyperbilirubinemia ManagementSara YousefAinda não há avaliações
- Hemorrhagic Disease of The NewbornDocumento3 páginasHemorrhagic Disease of The NewbornDevi SuryandariAinda não há avaliações
- Dr. Niranjan Murthy HL Associate Professor Dept of Physiology SSMC, TumkurDocumento53 páginasDr. Niranjan Murthy HL Associate Professor Dept of Physiology SSMC, TumkurnirilibAinda não há avaliações
- Fetal MonitoringDocumento6 páginasFetal MonitoringRraouzmaaliAinda não há avaliações
- Impey Obs and Gynae Revision Notes PDFDocumento9 páginasImpey Obs and Gynae Revision Notes PDFRoiseAinda não há avaliações
- Approach To Neonatal HyperbilirubinemiaDocumento34 páginasApproach To Neonatal HyperbilirubinemiaNilesh HatzadeAinda não há avaliações
- Green Top Guidelines 7Documento34 páginasGreen Top Guidelines 7garfield1Ainda não há avaliações
- Uterine FibroidsDocumento47 páginasUterine FibroidsMoh Aldhy HusaintAinda não há avaliações
- Hypertension in PregnancyDocumento34 páginasHypertension in PregnancyMusekhirAinda não há avaliações
- Keyes Neonatal Emergencies FinalDocumento108 páginasKeyes Neonatal Emergencies FinalthanyunAinda não há avaliações
- (Gyne) 2.1 PCOS, Hyperandrogenism & Hyperprolactenemia (OnaCruz) - WiniDocumento10 páginas(Gyne) 2.1 PCOS, Hyperandrogenism & Hyperprolactenemia (OnaCruz) - WiniDexter IanAinda não há avaliações
- Case History Ob & Gyne 4Documento6 páginasCase History Ob & Gyne 4maksventileAinda não há avaliações
- Abnormal Uterine Bleeding: - Rou'a Eyad - Rahaf EyadDocumento35 páginasAbnormal Uterine Bleeding: - Rou'a Eyad - Rahaf EyadYazeed Asrawi0% (1)
- Hemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUDocumento27 páginasHemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUAbdisalan hassanAinda não há avaliações
- Sepsis Neonatal 2012 PeiatricsDocumento12 páginasSepsis Neonatal 2012 PeiatricsWalter LojaAinda não há avaliações
- Abnormal Uterine Bleeding (AUB)Documento45 páginasAbnormal Uterine Bleeding (AUB)asdf0% (1)
- Renal Disease in PregnancyDocumento28 páginasRenal Disease in PregnancysuperjaxxxonAinda não há avaliações
- Obstetrics, Gynaecology-Textbook of Obstetrics and Gynaecology For Medical Students, 2nd Edition-Akin Agboola-2006Documento559 páginasObstetrics, Gynaecology-Textbook of Obstetrics and Gynaecology For Medical Students, 2nd Edition-Akin Agboola-2006fagiy51113Ainda não há avaliações
- Overview of Postpartum Hemorrhage - UpToDateDocumento48 páginasOverview of Postpartum Hemorrhage - UpToDatewendy100% (1)
- Nancy E Fay MD Facog Division of Reproductive MedicineDocumento32 páginasNancy E Fay MD Facog Division of Reproductive MedicineAdityo MulyonoAinda não há avaliações
- ALARMER Dystocia PDFDocumento5 páginasALARMER Dystocia PDFwilliamAinda não há avaliações
- Disseminated Intravascular CoagulationDocumento16 páginasDisseminated Intravascular CoagulationDocRNAinda não há avaliações
- Maternal Collapse During PregnancyDocumento57 páginasMaternal Collapse During PregnancytapayanaAinda não há avaliações
- Handbook of Current and Novel Protocols for the Treatment of InfertilityNo EverandHandbook of Current and Novel Protocols for the Treatment of InfertilityMichael H. DahanAinda não há avaliações
- 2023 OB/GYN Coding Manual: Components of Correct CodingNo Everand2023 OB/GYN Coding Manual: Components of Correct CodingAinda não há avaliações
- Eua Biocerna Sars Euasum 0Documento7 páginasEua Biocerna Sars Euasum 0Osama BakheetAinda não há avaliações
- 9Documento13 páginas9Osama BakheetAinda não há avaliações
- 9Documento13 páginas9Osama BakheetAinda não há avaliações
- Aborashad 2010 - Edit by Bosha11-4Documento96 páginasAborashad 2010 - Edit by Bosha11-4Osama BakheetAinda não há avaliações
- كيفية الحصول على شهادة البورد الامريكى للجمعية الأمريكية للكلينيكال باثولوجيDocumento11 páginasكيفية الحصول على شهادة البورد الامريكى للجمعية الأمريكية للكلينيكال باثولوجيOsama BakheetAinda não há avaliações
- New England Journal Medicine: The ofDocumento12 páginasNew England Journal Medicine: The ofOsama BakheetAinda não há avaliações
- 7Documento11 páginas7OSAMAAinda não há avaliações
- 182+سؤال+Documento27 páginas182+سؤال+Mohsen HaleemAinda não há avaliações
- Pembrolizumab Versus Docetaxel For Previously Treated, PD-L1-positive, Advanced Non-Small-Cell Lung Cancer (KEYNOTE-010) : A Randomised Controlled TrialDocumento12 páginasPembrolizumab Versus Docetaxel For Previously Treated, PD-L1-positive, Advanced Non-Small-Cell Lung Cancer (KEYNOTE-010) : A Randomised Controlled TrialOSAMAAinda não há avaliações
- 1Documento11 páginas1Osama BakheetAinda não há avaliações
- Lipids MetabolismDocumento19 páginasLipids MetabolismOsama BakheetAinda não há avaliações
- كيفية الحصول على شهادة البورد الامريكى للجمعية الأمريكية للكلينيكال باثولوجيDocumento11 páginasكيفية الحصول على شهادة البورد الامريكى للجمعية الأمريكية للكلينيكال باثولوجيOsama BakheetAinda não há avaliações
- 2001 Pathology MCQDocumento11 páginas2001 Pathology MCQOsama Bakheet100% (1)
- Practical Ielts Strategies 5 Test Practice Book 2015 An Insanely Dangerous Activities 5Documento3 páginasPractical Ielts Strategies 5 Test Practice Book 2015 An Insanely Dangerous Activities 5Osama Bakheet100% (1)
- كيفية الحصول على شهادة البورد الامريكى للجمعية الأمريكية للكلينيكال باثولوجيDocumento11 páginasكيفية الحصول على شهادة البورد الامريكى للجمعية الأمريكية للكلينيكال باثولوجيOsama BakheetAinda não há avaliações
- MCQ in Microbiology Immunology Questions and Answers With ExplanationDocumento4 páginasMCQ in Microbiology Immunology Questions and Answers With ExplanationOsama Bakheet50% (2)
- 1grammar For IeltsDocumento71 páginas1grammar For IeltsPaul Stato88% (8)
- Mrsa in Latin AmericaDocumento12 páginasMrsa in Latin AmericaOsama BakheetAinda não há avaliações
- MCB101 Introductory Microbiology LabDocumento8 páginasMCB101 Introductory Microbiology LabOsama BakheetAinda não há avaliações
- Isolation of NeisseriaDocumento2 páginasIsolation of NeisseriaOsama Bakheet100% (1)
- Microbiology MR - VP Flashcards - QuizletDocumento4 páginasMicrobiology MR - VP Flashcards - QuizletOsama BakheetAinda não há avaliações
- Install Acrobatupd11021 First Install Acrobatupd11022 AfterDocumento1 páginaInstall Acrobatupd11021 First Install Acrobatupd11022 AfterOsama BakheetAinda não há avaliações
- Cross Matching Tests: Routine vs. Urgent Compatibility ProceduresDocumento2 páginasCross Matching Tests: Routine vs. Urgent Compatibility ProceduresOsama BakheetAinda não há avaliações
- BacteDocumento13 páginasBacteAdriana GarciaAinda não há avaliações
- Neisseria - Denise PDFDocumento2 páginasNeisseria - Denise PDFOsama BakheetAinda não há avaliações
- Analyzing Microbes Manual of Molecular Biology TechniquesDocumento367 páginasAnalyzing Microbes Manual of Molecular Biology TechniquesOsama BakheetAinda não há avaliações
- Urinalysis SlidesDocumento10 páginasUrinalysis SlidesOsama BakheetAinda não há avaliações
- User Manual Ed 6 July 09Documento34 páginasUser Manual Ed 6 July 09Osama BakheetAinda não há avaliações
- Molecular Biology BOC.Documento12 páginasMolecular Biology BOC.Osama BakheetAinda não há avaliações
- StoolDocumento1 páginaStoolAhmed J AlhindaweAinda não há avaliações
- Glossary in MeotrologyDocumento31 páginasGlossary in Meotrologypanget ako100% (1)
- GM Aid - Random Encounters - Generic RPGDocumento1 páginaGM Aid - Random Encounters - Generic RPGDon PerryAinda não há avaliações
- Report Text AssignmentDocumento5 páginasReport Text Assignmenthirodian nurul faziraAinda não há avaliações
- Glossary of TurbineDocumento5 páginasGlossary of TurbinevesselAinda não há avaliações
- Physics EssayDocumento1 páginaPhysics EssayJLLOW GtAinda não há avaliações
- AH Lec - 8Documento25 páginasAH Lec - 8Sajjad HussainAinda não há avaliações
- K. Subramanya - Engineering Hy-Hill Education (India) (2009) 116 PDFDocumento1 páginaK. Subramanya - Engineering Hy-Hill Education (India) (2009) 116 PDFcivilengeeAinda não há avaliações
- Huong Dan Ki NangDocumento16 páginasHuong Dan Ki NangHuongThao PhamAinda não há avaliações
- AICE Marine - Unit 7 Test Questions/ Study Guide: (Answers)Documento19 páginasAICE Marine - Unit 7 Test Questions/ Study Guide: (Answers)philip 6969Ainda não há avaliações
- Fema P-320 2014 508 PDFDocumento71 páginasFema P-320 2014 508 PDFMateus Azevedo100% (1)
- Analisis Luas Daerah Proteksi Petir Jenis Early Streamer Pada Tower SuttDocumento11 páginasAnalisis Luas Daerah Proteksi Petir Jenis Early Streamer Pada Tower SuttaprilianaAinda não há avaliações
- Cooling Pond DesignDocumento3 páginasCooling Pond DesignKristel LenonAinda não há avaliações
- Dirr-112 Week 11-19 by KuyajovertDocumento10 páginasDirr-112 Week 11-19 by KuyajovertRobert Macalanao100% (4)
- Report TextDocumento4 páginasReport TextDaffaandhika PutraAinda não há avaliações
- SnowtamDocumento1 páginaSnowtamchofuan100% (1)
- Beaufort Wind ScaleDocumento2 páginasBeaufort Wind Scalerizzo8Ainda não há avaliações
- To Whom It May Concern: This Is To Certify That, of Legal Age Filipino, Married and A BonifideDocumento2 páginasTo Whom It May Concern: This Is To Certify That, of Legal Age Filipino, Married and A BonifideKathleen Shei Dela CruzAinda não há avaliações
- Temperature, Buoyancy, and Vertical Motion What Air Temperature?Documento7 páginasTemperature, Buoyancy, and Vertical Motion What Air Temperature?Salam AlbaradieAinda não há avaliações
- 1.30.12 Article - Tsunami PDFDocumento6 páginas1.30.12 Article - Tsunami PDFMrityunjay Kumar RaiAinda não há avaliações
- Name:-Shubham Kumar RAI Submitted To: - Shivapriya MamDocumento22 páginasName:-Shubham Kumar RAI Submitted To: - Shivapriya MamVipin Kumar RaiAinda não há avaliações
- Ship's Pivot Point and Forces that Affect Its LocationDocumento41 páginasShip's Pivot Point and Forces that Affect Its Locationbehzad parsi100% (1)
- V. Topalov's sporting journey analyzedDocumento13 páginasV. Topalov's sporting journey analyzedJuan Andres AuernheimerAinda não há avaliações
- Land and Sea Breeze WorksheetDocumento2 páginasLand and Sea Breeze Worksheetmark joseph cometa100% (1)
- 2022 Midterm Exam Earth and Life ScienceDocumento7 páginas2022 Midterm Exam Earth and Life ScienceKristian Jay NantaAinda não há avaliações
- Oral Com RoleplayDocumento4 páginasOral Com RoleplaypolidomariagemmaAinda não há avaliações
- Storm Z2 Rev4Documento20 páginasStorm Z2 Rev4TahirJabbarAinda não há avaliações
- Amortisseur WindingDocumento1 páginaAmortisseur Windingjsrplc7952Ainda não há avaliações
- The complete Sicilian Dragon black repertoireDocumento88 páginasThe complete Sicilian Dragon black repertoireDaniel's Jack67% (3)
- Climate Change - National Wildlife FederationDocumento9 páginasClimate Change - National Wildlife FederationSuresh MohanAinda não há avaliações
- 15 Mbmf-65-18dde-In PDFDocumento3 páginas15 Mbmf-65-18dde-In PDFРоманКочневAinda não há avaliações