Você também pode gostar
- In The Classroom Study Strategies: Better GradesDocumento4 páginasIn The Classroom Study Strategies: Better GradesAloah122346100% (1)
- Mar&Sept 2012Documento15 páginasMar&Sept 2012Farrukh Ali KhanAinda não há avaliações
- OBS &GYN EXAM QUESTIONSDocumento265 páginasOBS &GYN EXAM QUESTIONSreza_adrian_2100% (2)
- The Handbook of Continuing Professional Development For The Health IT ProfessionalDocumento315 páginasThe Handbook of Continuing Professional Development For The Health IT ProfessionalAloah122346100% (2)
- Part I سنه القمله 2016Documento20 páginasPart I سنه القمله 2016Aloah122346Ainda não há avaliações
- Mar&Sept 2012Documento15 páginasMar&Sept 2012Farrukh Ali KhanAinda não há avaliações
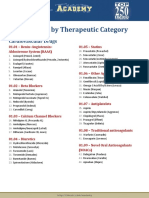
- Drug List by Therapeutic Category: Cardiovascular DrugsDocumento7 páginasDrug List by Therapeutic Category: Cardiovascular DrugsAloah122346Ainda não há avaliações
- Bacteria PDFDocumento13 páginasBacteria PDFJohn Christopher LucesAinda não há avaliações
- Semi Final Exam Saudi BoardDocumento6 páginasSemi Final Exam Saudi BoardAloah122346Ainda não há avaliações
- Online Contraceptive Information SurveyDocumento15 páginasOnline Contraceptive Information SurveyAloah122346Ainda não há avaliações
- Mohsen AttiaDocumento3 páginasMohsen AttiaAloah122346100% (1)
- Obstetric and Gynecology: A. ColpotomyDocumento44 páginasObstetric and Gynecology: A. ColpotomyAloah122346100% (1)
- Semi Final Exam Saudi BoardDocumento6 páginasSemi Final Exam Saudi BoardAloah122346Ainda não há avaliações
- Diagnosis and Management of Ectopic Pregnancy GuidelineDocumento41 páginasDiagnosis and Management of Ectopic Pregnancy GuidelineJose Luis Morales BautistaAinda não há avaliações
- Saudi Board OSCE2015Documento8 páginasSaudi Board OSCE2015Aloah122346Ainda não há avaliações
- Promotion 2013-2014 With AnswerDocumento36 páginasPromotion 2013-2014 With AnswerAloah122346Ainda não há avaliações
- Pre-NEET Obstetrics and Gynaecology (Sakshi Arora)Documento321 páginasPre-NEET Obstetrics and Gynaecology (Sakshi Arora)sipra jagu100% (4)
- Saudi Board OSCE2015Documento8 páginasSaudi Board OSCE2015Aloah122346Ainda não há avaliações
- Obstetric and Gynecology: A. ColpotomyDocumento44 páginasObstetric and Gynecology: A. ColpotomyAloah122346100% (1)
- Ethics Handbook For Residents PDFDocumento254 páginasEthics Handbook For Residents PDFAloah122346Ainda não há avaliações
- Pre NEET Obstetrics and Gynaecology (2013) (PDF) (UnitedVRG)Documento320 páginasPre NEET Obstetrics and Gynaecology (2013) (PDF) (UnitedVRG)Aloah122346100% (2)
- GTG 36 PDFDocumento13 páginasGTG 36 PDFAloah122346Ainda não há avaliações
- 1 PromtionDocumento14 páginas1 PromtionAloah122346Ainda não há avaliações
- LONDON Visitor GuideDocumento9 páginasLONDON Visitor GuideAndré Medeiros SztutmanAinda não há avaliações
- Saudi Board Exam 2015: These Answers Are Mine, They May Be Right, May Be WrongDocumento22 páginasSaudi Board Exam 2015: These Answers Are Mine, They May Be Right, May Be WrongAloah122346Ainda não há avaliações
- Final Exam Saudi Board 2009Documento38 páginasFinal Exam Saudi Board 2009Aloah122346Ainda não há avaliações
- Promotion OBGYNDocumento30 páginasPromotion OBGYNAloah122346Ainda não há avaliações
- 1 - Pelvic Anatomy PrimerDocumento44 páginas1 - Pelvic Anatomy PrimerAloah122346Ainda não há avaliações
- WHO Handbook of Blood TranfusionDocumento344 páginasWHO Handbook of Blood TranfusionWan Zafirah100% (1)
- ASRM AmenoreaDocumento7 páginasASRM AmenoreaTri GunawanAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Psychiatric Mental Health Nursing SuccessDocumento407 páginasPsychiatric Mental Health Nursing Successwhatever1919191986% (49)
- The Use of Glucommanan Flour From Gembili Tuber (Dioscorea Esculenta L.) As Gelling Agent in Chicken SausagesDocumento11 páginasThe Use of Glucommanan Flour From Gembili Tuber (Dioscorea Esculenta L.) As Gelling Agent in Chicken SausagesFadhil IkramAinda não há avaliações
- NUR1204-RLE - Group 4 - Home Visit Activity (HTP and HVP)Documento16 páginasNUR1204-RLE - Group 4 - Home Visit Activity (HTP and HVP)Jayvee BillonesAinda não há avaliações
- FM 999-3 Counter-Zombie Operations at The Fireteam Level v1.1Documento16 páginasFM 999-3 Counter-Zombie Operations at The Fireteam Level v1.1Arthur BarieAinda não há avaliações
- Pilar College Individual Nominee FormDocumento2 páginasPilar College Individual Nominee FormDes CuenoAinda não há avaliações
- Alan Palmieri ArticlesDocumento9 páginasAlan Palmieri Articleschris_blair_1Ainda não há avaliações
- Brady J. - Environmental Management in Organizations. The IEMA Handbook (2005)Documento459 páginasBrady J. - Environmental Management in Organizations. The IEMA Handbook (2005)Wan Naqib Hamidon100% (5)
- Handbook of Evidence-Based Radiation Oncology PDFDocumento756 páginasHandbook of Evidence-Based Radiation Oncology PDFDanielAinda não há avaliações
- A - An - The - No Article. ExercisesDocumento6 páginasA - An - The - No Article. ExercisesJoel Vilca YalleAinda não há avaliações
- Shell & Tube JSA PDFDocumento6 páginasShell & Tube JSA PDFAwinanto SaunAinda não há avaliações
- Liposomal IronDocumento6 páginasLiposomal IronPiyush KhetrapalAinda não há avaliações
- OCI Inventario Obsesivo Compulsivo (Foa, 2002)Documento11 páginasOCI Inventario Obsesivo Compulsivo (Foa, 2002)Margarita100% (1)
- Guiasgold2023 16235v2.1 Es-Pocket WMVDocumento55 páginasGuiasgold2023 16235v2.1 Es-Pocket WMVFABIO JAVIER BRAVO SALDARRIAGAAinda não há avaliações
- Final List of All MFG UnitDocumento123 páginasFinal List of All MFG UnitUdit MehraAinda não há avaliações
- Case Study Myocardial InfarctionDocumento23 páginasCase Study Myocardial InfarctionJester GalayAinda não há avaliações
- Personal Data Sheet: Marcial Roel FranciscoDocumento13 páginasPersonal Data Sheet: Marcial Roel FranciscoRoel MarcialAinda não há avaliações
- Family Context of Mental Health Risk in Tsunami-Exposed AdolescentsDocumento11 páginasFamily Context of Mental Health Risk in Tsunami-Exposed AdolescentsVirgílio BaltasarAinda não há avaliações
- Installation and Preoperative TestDocumento27 páginasInstallation and Preoperative TestLeonardo BaiaoAinda não há avaliações
- SPECIAL WORKSHOP ANNOUNCEMENT-with Keshe NotesDocumento4 páginasSPECIAL WORKSHOP ANNOUNCEMENT-with Keshe NotesAhmad AriesandyAinda não há avaliações
- PLR CourseDocumento43 páginasPLR CourseTaniya ChatterjeeAinda não há avaliações
- 12 MR - Norhisam Omar, Sales Manager, South East Asia of TenCate Geosynthetics Asia SDN BHDDocumento4 páginas12 MR - Norhisam Omar, Sales Manager, South East Asia of TenCate Geosynthetics Asia SDN BHDMuhammad FaisalAinda não há avaliações
- Anatomy Trains 3rd Edition Emag 1Documento62 páginasAnatomy Trains 3rd Edition Emag 1Dibyendu BanerjeeAinda não há avaliações
- Demystifying Buprenorphine Regulations For Pharmacists and CliniciansDocumento10 páginasDemystifying Buprenorphine Regulations For Pharmacists and Clinicianslorien86Ainda não há avaliações
- Team Performance ModelDocumento17 páginasTeam Performance ModelAdewumi Samson Segun100% (1)
- Nurses Role Fire and DisasterDocumento25 páginasNurses Role Fire and DisasterchellczyAinda não há avaliações
- 5G Connectivity and Its Effects in NigeriaDocumento15 páginas5G Connectivity and Its Effects in NigeriastephendivineoluwaseunAinda não há avaliações
- Nursing Care PlanDocumento3 páginasNursing Care PlanMarielle SorianoAinda não há avaliações
- The Human Body EnergyDocumento4 páginasThe Human Body EnergyOdette Müller-Dogan100% (3)
- I Srednje TestoviDocumento7 páginasI Srednje TestoviTatjana Stankovic SavicAinda não há avaliações
- Dody Firmanda 2009 - KPIs RS Krakatau Medika 6 Agustus 2009Documento40 páginasDody Firmanda 2009 - KPIs RS Krakatau Medika 6 Agustus 2009Dody Firmanda100% (6)