Você também pode gostar
- Final Impacted Third Molars-1Documento62 páginasFinal Impacted Third Molars-1Anam ShaikhAinda não há avaliações
- Treatment Planning Single Maxillary Anterior Implants for DentistsNo EverandTreatment Planning Single Maxillary Anterior Implants for DentistsAinda não há avaliações
- Fixed Orthodontic Appliances: A Practical GuideNo EverandFixed Orthodontic Appliances: A Practical GuideNota: 1 de 5 estrelas1/5 (1)
- Canine ImpactionDocumento31 páginasCanine Impactionavanthika krishnarajAinda não há avaliações
- Presented By: Assistant Professor:: M.R. Vatankhah Dr. H. M.SadeghiDocumento36 páginasPresented By: Assistant Professor:: M.R. Vatankhah Dr. H. M.SadeghiMuhammed HassanAinda não há avaliações
- Management of Impacted TeethDocumento153 páginasManagement of Impacted TeethToma Irina100% (1)
- 3D Teeth ReconstructionDocumento0 página3D Teeth ReconstructionSamir Alberita KeljmendiAinda não há avaliações
- Orthodontic Supplies CatalogDocumento320 páginasOrthodontic Supplies CatalogOrtho OrganizersAinda não há avaliações
- Anchorage SeminarDocumento14 páginasAnchorage Seminarঅরূপরতনবিশ্বাসAinda não há avaliações
- Methods of Gaining Space PDFDocumento5 páginasMethods of Gaining Space PDFFernaz BehlimAinda não há avaliações
- Model Analysis OrthoDocumento48 páginasModel Analysis OrthoFourthMolar.comAinda não há avaliações
- Dentosphere - World of Dentistry - MCQs On Skin and Vesiculobullous Diseases - Or-SearchableDocumento22 páginasDentosphere - World of Dentistry - MCQs On Skin and Vesiculobullous Diseases - Or-SearchableAssssssAinda não há avaliações
- 18-22 SlotDocumento10 páginas18-22 SlotchinnipragnaAinda não há avaliações
- Mccracken'S Removable Partial Prosthodontics. Chapter 10 & 19Documento50 páginasMccracken'S Removable Partial Prosthodontics. Chapter 10 & 19Al CarLozAinda não há avaliações
- Diagnosis of Canine ImpactionDocumento27 páginasDiagnosis of Canine ImpactionDr.Thrivikhraman KothandaramanAinda não há avaliações
- Indications and Contraindications For Rpa &rpi (Group 3)Documento10 páginasIndications and Contraindications For Rpa &rpi (Group 3)sidney changiAinda não há avaliações
- Class Iii Malocclusion: Yeoh Wen Li Iv Year Bds Roll No 35Documento40 páginasClass Iii Malocclusion: Yeoh Wen Li Iv Year Bds Roll No 35Yeoh Wen LiAinda não há avaliações
- Viva Questions in OrthodonticsDocumento4 páginasViva Questions in OrthodonticszainaAinda não há avaliações
- Biological Consideration in Mandibular Impression ProceduresDocumento41 páginasBiological Consideration in Mandibular Impression ProceduresSaravanan Thangarajan67% (3)
- Space ManagementDocumento11 páginasSpace Managementdr parveen bathla100% (1)
- Treatment PlanningDocumento28 páginasTreatment PlanningBimalKrishnaAinda não há avaliações
- Impacted Maxillary CanineDocumento8 páginasImpacted Maxillary CanineMatin Ahmad Khan100% (1)
- 31 SJ BDJ 2014 953Documento7 páginas31 SJ BDJ 2014 953Juan Augusto Fernández TarazonaAinda não há avaliações
- Smile Aesthetics in ProsthodonticsDocumento4 páginasSmile Aesthetics in Prosthodonticschai ling LoAinda não há avaliações
- Abutment Evaluation in FPD 2Documento5 páginasAbutment Evaluation in FPD 2ahmad955mlsAinda não há avaliações
- NATIONAL DENTAL BOARDS (NDB) / PART I: Passbooks Study GuideNo EverandNATIONAL DENTAL BOARDS (NDB) / PART I: Passbooks Study GuideNota: 1 de 5 estrelas1/5 (1)
- 3D-CT Evaluation of Facial Asymmetry in Patients With Maxillofacial DeformitiesDocumento9 páginas3D-CT Evaluation of Facial Asymmetry in Patients With Maxillofacial DeformitiesR KAinda não há avaliações
- Philosophy of Occlusion Past and Present. FOTOSDocumento10 páginasPhilosophy of Occlusion Past and Present. FOTOSMartha Lia Castaño EcheverryAinda não há avaliações
- Impacted Canine: Presented By: Dr. Ahmed Shihab Supervised By: Dr. SarahDocumento34 páginasImpacted Canine: Presented By: Dr. Ahmed Shihab Supervised By: Dr. SarahAhmed ShihabAinda não há avaliações
- Class II Amalgam PreparationDocumento41 páginasClass II Amalgam PreparationHanan MohAinda não há avaliações
- Development of Dentition and Occlusion - Dr. Nabil Al-ZubairDocumento124 páginasDevelopment of Dentition and Occlusion - Dr. Nabil Al-ZubairNabil Al-Zubair75% (4)
- 04 Splintstrismus 140501160338 Phpapp02Documento56 páginas04 Splintstrismus 140501160338 Phpapp02hazeemmegahedAinda não há avaliações
- Ceramics Overview Micro Proc MethodsDocumento13 páginasCeramics Overview Micro Proc MethodsAndreea IoanaAinda não há avaliações
- Teeth Arrangement Guidelines: by Saif Aldeen Salah AldeenDocumento16 páginasTeeth Arrangement Guidelines: by Saif Aldeen Salah AldeenDanna Rafiq100% (1)
- 7 Principles of Uncomplicated ExodontiaDocumento43 páginas7 Principles of Uncomplicated Exodontiaray774432Ainda não há avaliações
- Lec9 - Intra Oral Radiographic TechniquesDocumento13 páginasLec9 - Intra Oral Radiographic TechniquesSawsan Z. JwaiedAinda não há avaliações
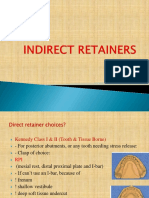
- Indirect RetainersDocumento52 páginasIndirect RetainerssarahAinda não há avaliações
- Bio Mechanics of Tooth MovementDocumento26 páginasBio Mechanics of Tooth MovementPriyanka WadhawanAinda não há avaliações
- Occlusion OrthodonticsDocumento84 páginasOcclusion OrthodonticsMuhammad UzairAinda não há avaliações
- Direct Indirect RetentionDocumento11 páginasDirect Indirect RetentionMaha LakshmiAinda não há avaliações
- Malocclusion Class IIIDocumento33 páginasMalocclusion Class IIIAyat KewanAinda não há avaliações
- Dynamic Nature of Lower Denture SpaceDocumento47 páginasDynamic Nature of Lower Denture SpacedrsanketcAinda não há avaliações
- Computer-Aided Designing and Computer-Aided Manufacturing in ProsthodonticsDocumento60 páginasComputer-Aided Designing and Computer-Aided Manufacturing in Prosthodonticsreshma shaikAinda não há avaliações
- Introduction To Composite RestorationsDocumento28 páginasIntroduction To Composite RestorationsAhmad Fawzi100% (2)
- Simple Tooth Extraction Technique: Amin AbusallamahDocumento35 páginasSimple Tooth Extraction Technique: Amin AbusallamahThiagoDaher100% (1)
- Fixed Orthodontic AppliancesDocumento45 páginasFixed Orthodontic AppliancesmuhammadmuktadirAinda não há avaliações
- SplintsDocumento3 páginasSplintsmuhammad naeem50% (2)
- Minor Oral Surgical Principles (NXPowerLite) / Orthodontic Courses by Indian Dental AcademyDocumento42 páginasMinor Oral Surgical Principles (NXPowerLite) / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Twin BlockDocumento124 páginasTwin Blockrama deviAinda não há avaliações
- Oral Wound Healing: Cell Biology and Clinical ManagementNo EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaAinda não há avaliações
- Transverse Dimension Andlong-Term Stability Robert L Vanarsdall JRDocumento10 páginasTransverse Dimension Andlong-Term Stability Robert L Vanarsdall JRMa Lyn GabayeronAinda não há avaliações
- Prostho Rehabilitation - HypodontiaDocumento24 páginasProstho Rehabilitation - HypodontiaAmniAzmiAinda não há avaliações
- Mixed DentitionDocumento49 páginasMixed Dentitiongnna norAinda não há avaliações
- Classification of Articulators: Awni Rihani, D.D.S., M.Sc.Documento4 páginasClassification of Articulators: Awni Rihani, D.D.S., M.Sc.Shanna MitchellAinda não há avaliações
- Orthodontic CurriculumDocumento60 páginasOrthodontic CurriculumKiran KumarAinda não há avaliações
- Rapid Maxillary Expansion and ApplianceDocumento4 páginasRapid Maxillary Expansion and Appliancedrzana78Ainda não há avaliações
- Poea FormDocumento1 páginaPoea FormNikkoCataquizAinda não há avaliações
- (DD13-14) Dental AnatomyDocumento443 páginas(DD13-14) Dental AnatomyJacobsen RichardAinda não há avaliações
- Corporation Law CasesDocumento1.509 páginasCorporation Law CasesNikkoCataquiz100% (1)
- 4 - Edward Nell v. Pacific FarmsDocumento4 páginas4 - Edward Nell v. Pacific FarmsStacy WheelerAinda não há avaliações
- Atrium Management Vs Court of Appeals Corp LawDocumento9 páginasAtrium Management Vs Court of Appeals Corp LawNikkoCataquizAinda não há avaliações
- Pci Bank Vs CA EscraDocumento29 páginasPci Bank Vs CA EscraNikkoCataquizAinda não há avaliações
- Intervention of Private Offended Party in Criminal ProceedingsDocumento1 páginaIntervention of Private Offended Party in Criminal ProceedingsNikkoCataquizAinda não há avaliações
- Legmed 101Documento9 páginasLegmed 101NikkoCataquizAinda não há avaliações
- Inquest, Remedies Available Before and After The Filing of An InformationDocumento2 páginasInquest, Remedies Available Before and After The Filing of An InformationNikkoCataquizAinda não há avaliações
- Determination of Probable Cause, Executive and JudicialDocumento1 páginaDetermination of Probable Cause, Executive and JudicialNikkoCataquiz100% (1)
- Crespo DoctrineDocumento1 páginaCrespo DoctrineNikkoCataquizAinda não há avaliações
- Legal Information: System RequirementsDocumento4 páginasLegal Information: System RequirementsAlex BogdanAinda não há avaliações
- Amendment of Information, Formal Vs SubstantialDocumento2 páginasAmendment of Information, Formal Vs SubstantialNikkoCataquiz100% (2)
- 50 CasesDocumento109 páginas50 CasesMaria FlorAinda não há avaliações
- Fernandez Vs Benjamin GreciaDocumento1 páginaFernandez Vs Benjamin GreciaNikkoCataquizAinda não há avaliações
- Stat ConDocumento4 páginasStat ConNikkoCataquizAinda não há avaliações
- Tollosa Vs Cargo C7Documento6 páginasTollosa Vs Cargo C7NikkoCataquizAinda não há avaliações
- RAYOS Vs Rayos Ombac c1-3Documento2 páginasRAYOS Vs Rayos Ombac c1-3NikkoCataquizAinda não há avaliações
- Ulep Vs The Legal Clinic C2Documento2 páginasUlep Vs The Legal Clinic C2NikkoCataquizAinda não há avaliações
- Talens-Dabon Vs Arceo C1-1Documento2 páginasTalens-Dabon Vs Arceo C1-1NikkoCataquiz100% (1)
- Terre Vs Terre C1-1Documento2 páginasTerre Vs Terre C1-1NikkoCataquizAinda não há avaliações
- Cayetano Vs Monsod SUMMARYDocumento2 páginasCayetano Vs Monsod SUMMARYNikkoCataquizAinda não há avaliações
- Law and Logic (Fallacies)Documento10 páginasLaw and Logic (Fallacies)Arbie Dela TorreAinda não há avaliações
- Compilation of Digest Consti1Documento22 páginasCompilation of Digest Consti1NikkoCataquizAinda não há avaliações
- Stat ConDocumento4 páginasStat ConNikkoCataquizAinda não há avaliações
- Outline of Constitutional Law 1 PDFDocumento29 páginasOutline of Constitutional Law 1 PDFNikkoCataquizAinda não há avaliações
- San Luis vs. San LuisDocumento2 páginasSan Luis vs. San LuisNikkoCataquizAinda não há avaliações
- SSS vs. BailonDocumento2 páginasSSS vs. BailonNikkoCataquizAinda não há avaliações
- Republic vs. NolascoDocumento2 páginasRepublic vs. NolascoNikkoCataquizAinda não há avaliações
- StoryboardTool 2Documento4 páginasStoryboardTool 2Majeda AbdAinda não há avaliações
- Pediatric Dyalisis Cases Book WaradyDocumento339 páginasPediatric Dyalisis Cases Book WaradyCinthya Quispe FernandezAinda não há avaliações
- Airway Assessment: Key PointsDocumento3 páginasAirway Assessment: Key PointsDr Olivia JacobAinda não há avaliações
- Reformatted Computed Tomography To Assess The Internal Nasal Valve and Association With Physical ExaminationDocumento6 páginasReformatted Computed Tomography To Assess The Internal Nasal Valve and Association With Physical ExaminationPutri HakimAinda não há avaliações
- Intracameral Mydriatics Versus Topical Mydriatics in Pupil Dilation For Phacoemulsification Cataract SurgeryDocumento5 páginasIntracameral Mydriatics Versus Topical Mydriatics in Pupil Dilation For Phacoemulsification Cataract SurgeryGlaucoma UnhasAinda não há avaliações
- Archiv Euromedica 06 2021 001 126 16 01 2022 13Documento6 páginasArchiv Euromedica 06 2021 001 126 16 01 2022 13Georgiana BuneaAinda não há avaliações
- Chandigarh DR IMADocumento13 páginasChandigarh DR IMADhruv VasudevaAinda não há avaliações
- June 2021 Case Census BlankDocumento2 páginasJune 2021 Case Census BlankJustitia Et PrudentiaAinda não há avaliações
- Careers Contacts - Virtual Fair v4Documento23 páginasCareers Contacts - Virtual Fair v4fidhaAinda não há avaliações
- 20 - Dec - 2023 - Kontraktur Digiti III Manus DextraDocumento12 páginas20 - Dec - 2023 - Kontraktur Digiti III Manus DextraAhmad Sahzul GaniAinda não há avaliações
- WNHS - OG.Arterial LineDocumento17 páginasWNHS - OG.Arterial LinePurwadi SujalmoAinda não há avaliações
- Obtaining Consent: A Clinical Guideline For The Diagnostic Imaging and Radiotherapy WorkforceDocumento19 páginasObtaining Consent: A Clinical Guideline For The Diagnostic Imaging and Radiotherapy Workforce박태용Ainda não há avaliações
- Perioperative Nursing ReportDocumento19 páginasPerioperative Nursing ReportPortia Dulce Patatag Toquero100% (1)
- Telescopes TontarraDocumento20 páginasTelescopes Tontarrag5quadAinda não há avaliações
- CCC Pgi Talk 2020 TransDocumento28 páginasCCC Pgi Talk 2020 TransDavid Cap33% (3)
- Letter of IntentDocumento1 páginaLetter of IntentMartin Capucion50% (2)
- Dressings: Carmina Disu Diana Ray Margarita DialaDocumento15 páginasDressings: Carmina Disu Diana Ray Margarita DialaNdor BariboloAinda não há avaliações
- Rehabilitation After Lumbar Discectomy, Microdiscectomy and Decompressive LaminectomyDocumento8 páginasRehabilitation After Lumbar Discectomy, Microdiscectomy and Decompressive LaminectomysilkofosAinda não há avaliações
- Lecture 7 - SterilizationDocumento12 páginasLecture 7 - SterilizationjemalAinda não há avaliações
- Periop 101 Study Guide #2Documento17 páginasPeriop 101 Study Guide #2Tawanda Boone-ShufordAinda não há avaliações
- Womac Hip Score (WHS) : Pain Severity (On Average) During The Past MonthDocumento3 páginasWomac Hip Score (WHS) : Pain Severity (On Average) During The Past MonthPetru CarajaAinda não há avaliações
- Neoplasma - Kelompok 1Documento46 páginasNeoplasma - Kelompok 1Echi KaruniaAinda não há avaliações
- SOPs For Infection Control and PreventionDocumento25 páginasSOPs For Infection Control and PreventionNoor ButtAinda não há avaliações
- Anatomy and Physiology of EyelidDocumento34 páginasAnatomy and Physiology of Eyelidsushma shrestha100% (1)
- Star Group Health InsuranceDocumento25 páginasStar Group Health InsuranceRUPESH VIJAYAKUMARAinda não há avaliações
- ResearchDocumento33 páginasResearchሌናፍ ኡሉምAinda não há avaliações
- Lawsuit Filed by Former Portland Timbers Goalkeeper Against Team DoctorsDocumento6 páginasLawsuit Filed by Former Portland Timbers Goalkeeper Against Team DoctorsKGW NewsAinda não há avaliações
- Clin Adv Periodontics - 2022 - Velasquez Plata - Osseous Topography in Biologically Driven Flap Design in MinimallyDocumento5 páginasClin Adv Periodontics - 2022 - Velasquez Plata - Osseous Topography in Biologically Driven Flap Design in Minimally安西 泰規Ainda não há avaliações
- ReportDocumento1 páginaReportAaRvi RvAinda não há avaliações
- Obgyn Flyeras4890Documento1 páginaObgyn Flyeras4890FirAinda não há avaliações