Você também pode gostar
- 2019 IL and Federal Pharmacy Law Review PDFDocumento176 páginas2019 IL and Federal Pharmacy Law Review PDFAnonymous 3YNJfYNQ100% (5)
- PHILHIS Executive Summary - EditedDocumento7 páginasPHILHIS Executive Summary - EditedMaxy Bariacto100% (1)
- Fibroblast Training Manual PORTALDocumento18 páginasFibroblast Training Manual PORTALElina MoralesAinda não há avaliações
- Project Report On Discontinuous Puf Panels Using Cyclopentane As A Blowing AgentDocumento6 páginasProject Report On Discontinuous Puf Panels Using Cyclopentane As A Blowing AgentEIRI Board of Consultants and PublishersAinda não há avaliações
- RA For Installation & Dismantling of Loading Platform A69Documento15 páginasRA For Installation & Dismantling of Loading Platform A69Sajid ShahAinda não há avaliações
- Integumentary SystemDocumento16 páginasIntegumentary Systemshenric16100% (8)
- Wound Care Gopi SirDocumento110 páginasWound Care Gopi SirArvind ShenoyAinda não há avaliações
- Wound CareDocumento10 páginasWound CareKenima Idao100% (3)
- RNSG 1413wounds Fall2006Documento67 páginasRNSG 1413wounds Fall2006api-3697326100% (1)
- Ns 313 Surgical Nursing: Wound Dressing TechniquesDocumento48 páginasNs 313 Surgical Nursing: Wound Dressing TechniquesZabron LuhendeAinda não há avaliações
- Trend and Issue in Wound Management: Dr. Suriadi, MSN, AwcsDocumento38 páginasTrend and Issue in Wound Management: Dr. Suriadi, MSN, AwcsfawwazAinda não há avaliações
- Principles of Wound Care: Professor Claire HaleDocumento20 páginasPrinciples of Wound Care: Professor Claire HaleMACPANAMERAAinda não há avaliações
- Integumentary System LectureDocumento157 páginasIntegumentary System LecturesnpjavierAinda não há avaliações
- Ern Mrcs Bk1Documento21 páginasErn Mrcs Bk1aeages100% (1)
- Assess and Diagnose the Integumentary SystemDocumento49 páginasAssess and Diagnose the Integumentary SystemAbdulla AshourAinda não há avaliações
- Pressure Ulcers: Francisco Torres Lozada MD Ponce Health Sciences University GeriatricsDocumento67 páginasPressure Ulcers: Francisco Torres Lozada MD Ponce Health Sciences University GeriatricsStephanie RiveraAinda não há avaliações
- Skin: Basic Structure and FunctionDocumento29 páginasSkin: Basic Structure and FunctionKrunal PatelAinda não há avaliações
- Wound Management ManualDocumento81 páginasWound Management ManualBrian Harris100% (2)
- Indonesian Wound Care Workbook for Certified Wound Care CliniciansDocumento12 páginasIndonesian Wound Care Workbook for Certified Wound Care CliniciansTakesi ArisandyAinda não há avaliações
- Trisha Sando Lecture on Wound Healing Stages and FactorsDocumento51 páginasTrisha Sando Lecture on Wound Healing Stages and FactorsMonasterio Tan KennethAinda não há avaliações
- Wound Care Education for StaffDocumento23 páginasWound Care Education for StaffMeagan Ristevski100% (1)
- The Integumentary System: Structure and FunctionDocumento54 páginasThe Integumentary System: Structure and FunctionStefanie Henry100% (1)
- BSN Nursing Practicum Focuses on Integumentary SystemDocumento10 páginasBSN Nursing Practicum Focuses on Integumentary SystemMichelle Gliselle Guinto MallareAinda não há avaliações
- The Skin Is An Organ of ProtectionDocumento5 páginasThe Skin Is An Organ of ProtectionFahmi Sulistyo HutomoAinda não há avaliações
- Skin Biology and Physiology BasicsDocumento31 páginasSkin Biology and Physiology BasicsprecyusmanAinda não há avaliações
- Wound CareDocumento17 páginasWound CareLestia AgustinaAinda não há avaliações
- Wound CareDocumento27 páginasWound Carepedrovsky702Ainda não há avaliações
- Uint No 6 Skin IntegretyDocumento23 páginasUint No 6 Skin Integretyeshasohaib92Ainda não há avaliações
- Chapter 6 WoundhealingDocumento41 páginasChapter 6 WoundhealingMelba AlanoAinda não há avaliações
- Wound CareDocumento17 páginasWound Caredlneisha6183% (6)
- Wound CareDocumento5 páginasWound CareEdgar Garcia100% (1)
- Wounds 1pptDocumento40 páginasWounds 1pptSachin KpAinda não há avaliações
- Pressure Ulcers: Problems and ChallengesDocumento23 páginasPressure Ulcers: Problems and Challengesedi edong100% (1)
- Discuss the role of growth factors and cytokines in wound healing processDocumento62 páginasDiscuss the role of growth factors and cytokines in wound healing processAnanda YulianAinda não há avaliações
- Wound Care Basics: Types, Staging, Assessment & TreatmentDocumento26 páginasWound Care Basics: Types, Staging, Assessment & TreatmentIntan Purnamasari100% (1)
- Wound Healing & Care Guide: Stages, Factors & TreatmentDocumento55 páginasWound Healing & Care Guide: Stages, Factors & TreatmentClaudio Luis VenturiniAinda não há avaliações
- Physical Changes in The Integumentary System As The Person AgesDocumento10 páginasPhysical Changes in The Integumentary System As The Person AgesDinarkram Rabreca EculAinda não há avaliações
- Case Pres PartDocumento12 páginasCase Pres PartJeannezelle Anne Mariz GazaAinda não há avaliações
- Anatomy and PhysiologyDocumento93 páginasAnatomy and PhysiologynonflashAinda não há avaliações
- Chapter 6 - IntegumentaryDocumento63 páginasChapter 6 - Integumentaryapi-297069611Ainda não há avaliações
- Clinical Protocol For Wound Management 2013Documento17 páginasClinical Protocol For Wound Management 2013Moloce BeatriceAinda não há avaliações
- Medical-Surgical Nursing: An Integrated Approach, 2E: Nursing Care of The Client: Integumentary SystemDocumento36 páginasMedical-Surgical Nursing: An Integrated Approach, 2E: Nursing Care of The Client: Integumentary Systemtanmai nooluAinda não há avaliações
- BurnsDocumento55 páginasBurnsMohammad Amjad KhanAinda não há avaliações
- Wound Management GuidelinesDocumento12 páginasWound Management GuidelinesFransiscus Braveno RapaAinda não há avaliações
- Handouts Integumentary Sys Sp11 B201Documento7 páginasHandouts Integumentary Sys Sp11 B201Kelly TrainorAinda não há avaliações
- ENT 219 - BIOMATERIALS ARTIFICIAL SKINDocumento34 páginasENT 219 - BIOMATERIALS ARTIFICIAL SKINMohâmmed Ä. ÃlFakihAinda não há avaliações
- Wound Healing Phases & Tissue RepairDocumento39 páginasWound Healing Phases & Tissue Repairjue_mardhiahAinda não há avaliações
- M13 - Dermatology - Chapter 1Documento10 páginasM13 - Dermatology - Chapter 1Idham BaharudinAinda não há avaliações
- Skin IntegrityDocumento112 páginasSkin IntegrityHerlina NababanAinda não há avaliações
- Referat - CHRONIC WOUNDDocumento19 páginasReferat - CHRONIC WOUNDAfifah Syifaul UmmahAinda não há avaliações
- 8-Wounds and Wound Healing-1Documento31 páginas8-Wounds and Wound Healing-1Aiden JosephatAinda não há avaliações
- Wound management stages healingDocumento14 páginasWound management stages healingnjoomAinda não há avaliações
- Asuhan Keperawatan Gangguan Sistem Integumentum Pada LansiaDocumento50 páginasAsuhan Keperawatan Gangguan Sistem Integumentum Pada LansiadwiinasAinda não há avaliações
- 1 Review of Wound Healing and Closure MethodsDocumento30 páginas1 Review of Wound Healing and Closure MethodsZhishanAinda não há avaliações
- Links For The Wound Care TopicDocumento6 páginasLinks For The Wound Care Topicericka.carnaceteAinda não há avaliações
- 420-510chapter 1 (5) Introduction To The Integumentary SystemDocumento6 páginas420-510chapter 1 (5) Introduction To The Integumentary Systemtomorrow.today.yesterday .yesterdayAinda não há avaliações
- Wound CareDocumento13 páginasWound CareZhayree R.Ainda não há avaliações
- Tissue Integrity Outline Spring 2023Documento25 páginasTissue Integrity Outline Spring 2023morganstorey0Ainda não há avaliações
- Wound Dressings Update: Carolina Weller, Geoff SussmanDocumento7 páginasWound Dressings Update: Carolina Weller, Geoff SussmanyodinheimAinda não há avaliações
- Phases of Burn Care: Emergent, Acute, RehabilitationDocumento3 páginasPhases of Burn Care: Emergent, Acute, RehabilitationhameunjungAinda não há avaliações
- Skin Integrity and Hygiene CareDocumento11 páginasSkin Integrity and Hygiene CareMaria Mika Ella RetizaAinda não há avaliações
- Exudate Management (Maserasi Dan HypergranulasiDocumento48 páginasExudate Management (Maserasi Dan HypergranulasiEza R. KusumaAinda não há avaliações
- Wound Healing: Stem Cells Repair and Restorations, Basic and Clinical AspectsNo EverandWound Healing: Stem Cells Repair and Restorations, Basic and Clinical AspectsAinda não há avaliações
- Evaluation FormDocumento2 páginasEvaluation Formcharity kalinowskyAinda não há avaliações
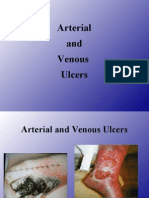
- 4 - Arterial & Venous UlcersDocumento86 páginas4 - Arterial & Venous Ulcerscharity kalinowsky100% (13)
- Metastatic WoundsDocumento112 páginasMetastatic Woundscharity kalinowsky100% (1)
- Diabetic Foot Ulcers Prevention & ManagementDocumento59 páginasDiabetic Foot Ulcers Prevention & Managementcharity kalinowsky100% (2)
- 2 - Pressure UlcersDocumento64 páginas2 - Pressure Ulcerscharity kalinowsky100% (5)
- Defining Public RelationsDocumento4 páginasDefining Public RelationsKARTAVYA SINGHAinda não há avaliações
- The Daily Tar Heel For September 18, 2012Documento8 páginasThe Daily Tar Heel For September 18, 2012The Daily Tar HeelAinda não há avaliações
- Bolt Jul 201598704967704 PDFDocumento136 páginasBolt Jul 201598704967704 PDFaaryangargAinda não há avaliações
- E.sybox - Esybox All Information PDFDocumento56 páginasE.sybox - Esybox All Information PDFnle_16948Ainda não há avaliações
- Acc418 2020 2Documento3 páginasAcc418 2020 2faithAinda não há avaliações
- SCM PPT (Supply Chain Management)Documento19 páginasSCM PPT (Supply Chain Management)Mairaj NaseemAinda não há avaliações
- CA-Endevor Quick EditDocumento31 páginasCA-Endevor Quick Editmariela mmascelloniAinda não há avaliações
- Electronics HubDocumento9 páginasElectronics HubKumaran SgAinda não há avaliações
- Security Testing MatDocumento9 páginasSecurity Testing MatLias JassiAinda não há avaliações
- OS9000 AOS 6.1.5 R01 Network Configuration GuideDocumento846 páginasOS9000 AOS 6.1.5 R01 Network Configuration GuideclaupasinaAinda não há avaliações
- Canopen-Lift Shaft Installation: W+W W+WDocumento20 páginasCanopen-Lift Shaft Installation: W+W W+WFERNSAinda não há avaliações
- Complete Approval List by FSSAIDocumento16 páginasComplete Approval List by FSSAIAnkush Pandey100% (1)
- DBIRS SyllabusDocumento2 páginasDBIRS SyllabusAshitosh KadamAinda não há avaliações
- Assignment 2Documento4 páginasAssignment 2maxamed0% (1)
- L P 10Documento13 páginasL P 10Bình Minh HoàngAinda não há avaliações
- Quality Management - QuestionDocumento4 páginasQuality Management - QuestionLawzy Elsadig SeddigAinda não há avaliações
- Toki PonaDocumento2 páginasToki PonaNicholas FletcherAinda não há avaliações
- HUMAN RIGHTS, RATIONALITY, AND SENTIMENTALITYDocumento13 páginasHUMAN RIGHTS, RATIONALITY, AND SENTIMENTALITYJohn HunterAinda não há avaliações
- Marketing Budget: Expenses Q1 Q2 Q3 Q4 Totals Budget %Documento20 páginasMarketing Budget: Expenses Q1 Q2 Q3 Q4 Totals Budget %Miaow MiaowAinda não há avaliações
- Project Planning and Management Unit 1Documento13 páginasProject Planning and Management Unit 1Savant100% (1)
- EMarketer Time Spent With Media SnapshotDocumento13 páginasEMarketer Time Spent With Media SnapshotWei ShingAinda não há avaliações
- T Cells & Autoimmunity, s3Documento21 páginasT Cells & Autoimmunity, s3LiaAriestaAinda não há avaliações
- Historical Source Author Date of The Event Objective of The Event Persons Involved Main ArgumentDocumento5 páginasHistorical Source Author Date of The Event Objective of The Event Persons Involved Main ArgumentMark Saldie RoncesvallesAinda não há avaliações
- Administrations whose CoCs are accepted for CECDocumento1 páginaAdministrations whose CoCs are accepted for CECGonçalo CruzeiroAinda não há avaliações
- Disappearance of Madeleine McCannDocumento36 páginasDisappearance of Madeleine McCannCopernicAinda não há avaliações
- Journal 082013Documento100 páginasJournal 082013Javier Farias Vera100% (1)