Você também pode gostar
- Neurobiology of Mental IllnessDocumento1.024 páginasNeurobiology of Mental IllnessMario Barragan Cortez100% (1)
- Hormone Replacement Therapy (HRT) Evidence-Based Guidelines: DR Mahdy El-Mazzahy Damietta General HospitalDocumento38 páginasHormone Replacement Therapy (HRT) Evidence-Based Guidelines: DR Mahdy El-Mazzahy Damietta General Hospitalhossam626Ainda não há avaliações
- Hospital: Ms .Neethu Vincent Asst Professor KVM College of NursingDocumento29 páginasHospital: Ms .Neethu Vincent Asst Professor KVM College of NursingNeethu VincentAinda não há avaliações
- Back PainDocumento110 páginasBack PainRushdaAinda não há avaliações
- Customer Satisfaction in HospitalsDocumento23 páginasCustomer Satisfaction in HospitalsanilsumanAinda não há avaliações
- Brain TumorDocumento30 páginasBrain TumorRushdaAinda não há avaliações
- Brain TumorDocumento30 páginasBrain TumorRushdaAinda não há avaliações
- 5 Reducing Time To Analgesia in The Emergency Department Using ADocumento10 páginas5 Reducing Time To Analgesia in The Emergency Department Using AMegaHandayaniAinda não há avaliações
- Pelvic Physical Therapy For Chronic Pain and Dysfunction FollowinDocumento13 páginasPelvic Physical Therapy For Chronic Pain and Dysfunction Followincode PVSAinda não há avaliações
- Hot Sitz Bath ReliefDocumento10 páginasHot Sitz Bath ReliefJohn Aladin ArcetaAinda não há avaliações
- Quality Management in HospitalDocumento16 páginasQuality Management in HospitalAr. Shruti GuptaAinda não há avaliações
- Financing and Delivery of Health Services NCMCHDocumento320 páginasFinancing and Delivery of Health Services NCMCHBrand SynapseAinda não há avaliações
- Dopamine Drug StudyDocumento6 páginasDopamine Drug StudyGeorge RussellAinda não há avaliações
- Chapter 5: Studying Disease DistributionDocumento7 páginasChapter 5: Studying Disease DistributionJohn Rick OrineAinda não há avaliações
- Aetcom LectureDocumento74 páginasAetcom LectureBittu Solanki100% (1)
- HospitalDocumento27 páginasHospitaljyothiAinda não há avaliações
- Histology of The Special SenseDocumento84 páginasHistology of The Special SenseRushdaAinda não há avaliações
- Hospital ManagementDocumento26 páginasHospital Managementsanjib beraAinda não há avaliações
- ACE Group Fitness Instructor Certification GuideDocumento36 páginasACE Group Fitness Instructor Certification GuideLouis TrầnAinda não há avaliações
- AETCOM QuestionairDocumento3 páginasAETCOM Questionairlatest techs&tips100% (1)
- Laboratory Services in HospitalDocumento58 páginasLaboratory Services in HospitalDr. Rakshit SolankiAinda não há avaliações
- Health Systems & Facilities Historical DevelopmentDocumento6 páginasHealth Systems & Facilities Historical DevelopmentMikee MeladAinda não há avaliações
- Scientific evidence for clinical use of horsetailDocumento23 páginasScientific evidence for clinical use of horsetailDanilo Maciel Carneiro100% (1)
- National Quality Assurance Standars - BlueDocumento64 páginasNational Quality Assurance Standars - Bluears_delAinda não há avaliações
- Customer Satisfaction and Service MarketingDocumento22 páginasCustomer Satisfaction and Service MarketingAnshita GargAinda não há avaliações
- Infectious Disease Outbreak RRM PDFDocumento75 páginasInfectious Disease Outbreak RRM PDFmichlsy11Ainda não há avaliações
- Role of Manager in HospitalDocumento16 páginasRole of Manager in HospitalPrasidha Prabhu100% (1)
- TubercolosisDocumento8 páginasTubercolosisNitesh Bhura100% (1)
- Medical Council of India introduces AETCOM module to strengthen attitude, ethics and communication competenciesDocumento94 páginasMedical Council of India introduces AETCOM module to strengthen attitude, ethics and communication competenciesSushanta100% (1)
- Pediatric Chemotherapy Administration: An OverviewDocumento76 páginasPediatric Chemotherapy Administration: An OverviewMiftaa HurrahmiAinda não há avaliações
- Summer Internship Project Report On (1) - 2Documento25 páginasSummer Internship Project Report On (1) - 2arshad khanAinda não há avaliações
- Ood Linical Ractice (GCP) in Clinical Research: Food and Drug AdministrationDocumento127 páginasOod Linical Ractice (GCP) in Clinical Research: Food and Drug AdministrationPap PipAinda não há avaliações
- Patient Satisfaction With Primary Healthcare in Kashmir IndiaDocumento12 páginasPatient Satisfaction With Primary Healthcare in Kashmir IndiaInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- Dominos Pizza Human ResourseDocumento39 páginasDominos Pizza Human ResourseVandita RannsinghAinda não há avaliações
- Design and Implementation of Computerized Hospital Database MNT SystemDocumento13 páginasDesign and Implementation of Computerized Hospital Database MNT SystemOgidiolu Temitope EbenezerAinda não há avaliações
- Patient Satisfaction Survey at Al-Nafees Hospital OPDDocumento6 páginasPatient Satisfaction Survey at Al-Nafees Hospital OPDapouakone apouakoneAinda não há avaliações
- Apollo Specialty HospitalDocumento30 páginasApollo Specialty HospitalAshwin Sudhakar100% (3)
- Service Quality Customer Satisfaction 2 PDFDocumento9 páginasService Quality Customer Satisfaction 2 PDFkelvin kristiantoAinda não há avaliações
- Indian Hospital SectorDocumento26 páginasIndian Hospital Sectorabhijitsamanta1Ainda não há avaliações
- MRD Meaning, FNDocumento22 páginasMRD Meaning, FNRiya Pinto100% (1)
- Patient Satisfaction With The Quality of Covid-19 Inpatient Service Based On The Servwual MethodDocumento9 páginasPatient Satisfaction With The Quality of Covid-19 Inpatient Service Based On The Servwual MethodEdi Yulia RamdanAinda não há avaliações
- Early Clinical Exposure (Ece)Documento30 páginasEarly Clinical Exposure (Ece)sandeepAinda não há avaliações
- DR Lal Path Labs LTD: Sub: Proposal For Pathology ServicesDocumento3 páginasDR Lal Path Labs LTD: Sub: Proposal For Pathology ServicesKavita BatraAinda não há avaliações
- QuizDocumento14 páginasQuizBalaji Operations ManagerAinda não há avaliações
- PGHHHMDocumento30 páginasPGHHHMDaipayan Lodh75% (4)
- Public Private Partnership in Health Care: Shiv Chandra MathurDocumento14 páginasPublic Private Partnership in Health Care: Shiv Chandra MathurUtpal DekaAinda não há avaliações
- Quality and HospitalDocumento6 páginasQuality and HospitalKuldeep BajajAinda não há avaliações
- Doctor Patient RelationshipDocumento4 páginasDoctor Patient RelationshipvishnuAinda não há avaliações
- A Meta Analysis of The Effects of Resistance Training On Blood S 2020 MidwifDocumento10 páginasA Meta Analysis of The Effects of Resistance Training On Blood S 2020 Midwifriska yolandaAinda não há avaliações
- Medical EthicsDocumento13 páginasMedical EthicsLizbeth Aura CebrianAinda não há avaliações
- Agents Used in AnemiasDocumento26 páginasAgents Used in AnemiasHajrahPalembangan100% (1)
- Medico-Legal Cases in IndiaDocumento2 páginasMedico-Legal Cases in Indiaaishwarya shetty100% (1)
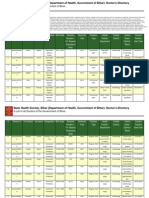
- DarbhangaDocumento31 páginasDarbhangadrpklalAinda não há avaliações
- Laws and Rules Governing HospitalsDocumento6 páginasLaws and Rules Governing HospitalsAnil BgAinda não há avaliações
- The Heath Care Delivery SystemDocumento17 páginasThe Heath Care Delivery SystemAngelou RosalesAinda não há avaliações
- DR Mogli 1Documento10 páginasDR Mogli 1pmm05479Ainda não há avaliações
- Bangladesh National Health Policy-2011Documento19 páginasBangladesh National Health Policy-2011Fairouz Khan100% (1)
- Pantone and K100 Reverse White MedicineDocumento16 páginasPantone and K100 Reverse White MedicinepaanarAinda não há avaliações
- Hospital - A Complex System With Integrated ComponentsDocumento4 páginasHospital - A Complex System With Integrated ComponentsSamAinda não há avaliações
- Introduction and Importance of Outcome MeasuresDocumento16 páginasIntroduction and Importance of Outcome MeasuresZoya KhanAinda não há avaliações
- Synopsis On Patient Safety in OPDDocumento6 páginasSynopsis On Patient Safety in OPDniceprachiAinda não há avaliações
- Patient Safety: What Should We Be Trying To Communicate?Documento32 páginasPatient Safety: What Should We Be Trying To Communicate?cicaklomenAinda não há avaliações
- To Find Out The Relationship Between Service Quality and Customer Satisfaction in HospitalsDocumento30 páginasTo Find Out The Relationship Between Service Quality and Customer Satisfaction in HospitalsAnonymous Bhnfli100% (1)
- Healthcare Quality Management CertificationDocumento8 páginasHealthcare Quality Management Certificationselinasimpson351Ainda não há avaliações
- HR Department at Desun HospitalDocumento17 páginasHR Department at Desun HospitalDIYA DINDAAinda não há avaliações
- Medical Negligence: Dr. Prateek RastogiDocumento19 páginasMedical Negligence: Dr. Prateek RastogiHarish AgarwalAinda não há avaliações
- DMLT Syllabus GuideDocumento2 páginasDMLT Syllabus Guideardhendubooks100% (1)
- EthicsDocumento65 páginasEthicsUmesh KawalkarAinda não há avaliações
- Sam PDFDocumento134 páginasSam PDFPunit Garg100% (2)
- The Doctor-Patient Relationship and Interviewing TechniquesDocumento50 páginasThe Doctor-Patient Relationship and Interviewing TechniquesPranay KumarAinda não há avaliações
- The Doctor-Patient RelationshipDocumento55 páginasThe Doctor-Patient RelationshipMuhammad NaveedAinda não há avaliações
- Doctor Patient RelationshipDocumento21 páginasDoctor Patient RelationshipPutri Rizky AmaliaAinda não há avaliações
- Tibia and Femur Shaft Fracture GuideDocumento21 páginasTibia and Femur Shaft Fracture GuideRushdaAinda não há avaliações
- Humeral Shaft Fracture DiscussionDocumento18 páginasHumeral Shaft Fracture DiscussionRushdaAinda não há avaliações
- Parathyroid TumorDocumento25 páginasParathyroid TumorRushdaAinda não há avaliações
- Eyelids AdnexalDocumento52 páginasEyelids AdnexalRushdaAinda não há avaliações
- Understanding HydrocephalusDocumento36 páginasUnderstanding HydrocephalusRushdaAinda não há avaliações
- Meningocele Dan MeningomyoceleDocumento10 páginasMeningocele Dan MeningomyoceleRushdaAinda não há avaliações
- DermatotherapyDocumento56 páginasDermatotherapyRushda100% (1)
- TraumaDocumento65 páginasTraumaRushdaAinda não há avaliações
- Scleral DiseasesDocumento40 páginasScleral DiseasesRushdaAinda não há avaliações
- Eye ComplicationsDocumento20 páginasEye ComplicationsRushdaAinda não há avaliações
- Hair DisorderDocumento49 páginasHair DisorderRushdaAinda não há avaliações
- KorneaDocumento50 páginasKorneaRushdaAinda não há avaliações
- Perioral DermatitisDocumento18 páginasPerioral DermatitisRushdaAinda não há avaliações
- RosaceaDocumento21 páginasRosaceaRushdaAinda não há avaliações
- GlaucomaDocumento47 páginasGlaucomaRushdaAinda não há avaliações
- UveitisDocumento25 páginasUveitisRushdaAinda não há avaliações
- SDHDocumento6 páginasSDHRushdaAinda não há avaliações
- HyperhidrosisDocumento69 páginasHyperhidrosisRushdaAinda não há avaliações
- Mata KorneaDocumento37 páginasMata KorneaRushdaAinda não há avaliações
- GINA Pocket 2015Documento32 páginasGINA Pocket 2015Ramzi AkramAinda não há avaliações
- Special Sense System Group 6Documento24 páginasSpecial Sense System Group 6RushdaAinda não há avaliações
- 8.refractive DisorderDocumento38 páginas8.refractive DisorderRushdaAinda não há avaliações
- Anatomy and Physiology of the Skin: Structure, Functions, and ProcessesDocumento23 páginasAnatomy and Physiology of the Skin: Structure, Functions, and ProcessesRushdaAinda não há avaliações
- At-A-Glance Outpatient Management Reference For Chronic Obstructive Pulmonary Disease (COPD)Documento8 páginasAt-A-Glance Outpatient Management Reference For Chronic Obstructive Pulmonary Disease (COPD)RushdaAinda não há avaliações
- Gupta RX Pityriasis Versicolor J Fungi 2015Documento17 páginasGupta RX Pityriasis Versicolor J Fungi 2015akuro imaizumiAinda não há avaliações
- Pityriasis VersicolorDocumento4 páginasPityriasis VersicolorRushdaAinda não há avaliações
- Gross Pathology SpringerDocumento2 páginasGross Pathology SpringerThalia ChristabelAinda não há avaliações
- Aesthetic Medicine Training CourseDocumento8 páginasAesthetic Medicine Training Coursedrdahabra3Ainda não há avaliações
- List of Books Box # 35: S.No. Author Title Year Edition Vol Call #Documento10 páginasList of Books Box # 35: S.No. Author Title Year Edition Vol Call #lubs123Ainda não há avaliações
- Circulating SerotoninDocumento17 páginasCirculating Serotoninnihilx27374Ainda não há avaliações
- II-Vocab of Hospital DeptDocumento1 páginaII-Vocab of Hospital DeptAdhwaAinda não há avaliações
- Safety Aspects of Probiotic ProductsDocumento4 páginasSafety Aspects of Probiotic ProductsSrinivas PingaliAinda não há avaliações
- Rule: Medicare: Physician Fee Schedule (CY 2007) Payment Policies and Relative Value UnitsDocumento629 páginasRule: Medicare: Physician Fee Schedule (CY 2007) Payment Policies and Relative Value UnitsJustia.com100% (1)
- Sarcopenia - Revised European Consensus On Definition and Diagnosis 2019Documento16 páginasSarcopenia - Revised European Consensus On Definition and Diagnosis 2019Matheus MartinsAinda não há avaliações
- Opportunistic MycosesDocumento13 páginasOpportunistic MycosesErnest CañosAinda não há avaliações
- List of Nanda Nursing Diagnosis 2012Documento6 páginasList of Nanda Nursing Diagnosis 2012Amit MartinAinda não há avaliações
- Brain Tissue Oxygen MonitoringDocumento11 páginasBrain Tissue Oxygen MonitoringangiolikkiaAinda não há avaliações
- Daftar Pustaka-Wps OfficeDocumento2 páginasDaftar Pustaka-Wps OfficeRezha July prakosoAinda não há avaliações
- Breathe. Exhale. Repeat - The Benefits of Controlled BreathingDocumento3 páginasBreathe. Exhale. Repeat - The Benefits of Controlled BreathingDaxten KienAinda não há avaliações
- 3rd BAMS 15 16 17Documento73 páginas3rd BAMS 15 16 17Nayan MaheshwariAinda não há avaliações
- Journal Terapi Dermatitis SeboroikDocumento4 páginasJournal Terapi Dermatitis SeboroikMohd Faie RamliAinda não há avaliações
- MudrasDocumento8 páginasMudrasKishore CheralaAinda não há avaliações
- Renal Failure in ChildrenDocumento43 páginasRenal Failure in Childrendennyyy175Ainda não há avaliações
- Eye DiagnosisDocumento10 páginasEye DiagnosisAfrah NajeebAinda não há avaliações
- Pulmonary Embolism: Presented By: Miss. M.K.Kaku Nursing TutorDocumento9 páginasPulmonary Embolism: Presented By: Miss. M.K.Kaku Nursing TutorKaku ManishaAinda não há avaliações
- Bilingual WYNK FilipinoDocumento96 páginasBilingual WYNK FilipinoKyla Reine DayagAinda não há avaliações
- Metoprolol and AmiodaroneDocumento5 páginasMetoprolol and AmiodaroneNolte BombayAinda não há avaliações
- Master Advisory MergedDocumento6 páginasMaster Advisory MergedMary Joy Tenorio CabantudAinda não há avaliações