Você também pode gostar
- Local Mechanisms Affect MAPDocumento1 páginaLocal Mechanisms Affect MAPJohnVincentPagadduAinda não há avaliações
- Fever Headache Dizziness Seizure Nausea Vomiting: - X Cough DOB Constipation Diarrhea - X Abd. Pain: Location: QualityDocumento2 páginasFever Headache Dizziness Seizure Nausea Vomiting: - X Cough DOB Constipation Diarrhea - X Abd. Pain: Location: QualityJohnVincentPagadduAinda não há avaliações
- Critical Appraisal by John Vincent Pagaddu, M.D.Documento91 páginasCritical Appraisal by John Vincent Pagaddu, M.D.JohnVincentPagadduAinda não há avaliações
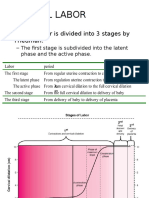
- Normal Labor: - Normal Labor Is Divided Into 3 Stages by FriedmanDocumento13 páginasNormal Labor: - Normal Labor Is Divided Into 3 Stages by FriedmanJohnVincentPagadduAinda não há avaliações
- Self-Reliance and ProcurementDocumento16 páginasSelf-Reliance and ProcurementJohnVincentPagadduAinda não há avaliações
- Systemic Response To InjuryDocumento15 páginasSystemic Response To InjuryJohnVincentPagaddu100% (1)
- Bio StatisticsDocumento16 páginasBio StatisticsJohnVincentPagadduAinda não há avaliações
- ENC Part IDocumento6 páginasENC Part IJohnVincentPagadduAinda não há avaliações
- Etiology: Pneumoniae. Nontypeable Haemophilus Influenzae and Moraxella Catarrhalis May Be Significant Pathogens inDocumento4 páginasEtiology: Pneumoniae. Nontypeable Haemophilus Influenzae and Moraxella Catarrhalis May Be Significant Pathogens inJohnVincentPagadduAinda não há avaliações
- HealthDocumento5 páginasHealthJohnVincentPagadduAinda não há avaliações
- Mollusc I Pox VirusDocumento2 páginasMollusc I Pox VirusJohnVincentPagadduAinda não há avaliações
- Population Mortality: Reported By: Group Four TFEG1 Biology 160 Lab AY 2010-2011 2 SemesterDocumento57 páginasPopulation Mortality: Reported By: Group Four TFEG1 Biology 160 Lab AY 2010-2011 2 SemesterJohnVincentPagadduAinda não há avaliações
- Derma Sample Exam For Practicals (Skin and Lesions)Documento42 páginasDerma Sample Exam For Practicals (Skin and Lesions)JohnVincentPagaddu100% (1)
- Sanctity and ScarcityDocumento33 páginasSanctity and ScarcityJohnVincentPagaddu100% (1)
- Types of Mixtures LabDocumento2 páginasTypes of Mixtures LabJohnVincentPagadduAinda não há avaliações
- Surgery Ortho TraumaDocumento8 páginasSurgery Ortho TraumaJohnVincentPagadduAinda não há avaliações
- Pediaortho Hand OutDocumento119 páginasPediaortho Hand OutJohnVincentPagadduAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- Introduction To Health PsychologyDocumento22 páginasIntroduction To Health PsychologyUm Ar100% (1)
- Anaphylactic ShockDocumento24 páginasAnaphylactic ShockEve Megan AbingAinda não há avaliações
- Bipolar DisordersDocumento63 páginasBipolar DisorderselvinegunawanAinda não há avaliações
- What Is FOOD?Documento27 páginasWhat Is FOOD?Naimul Haque NayeemAinda não há avaliações
- Trigger Point InjectionDocumento10 páginasTrigger Point Injectionv_vijayakanth7656Ainda não há avaliações
- Approach To Movement Disorders ..Documento54 páginasApproach To Movement Disorders ..Ihda ParidahAinda não há avaliações
- ReviewerDocumento20 páginasReviewerkriziahdonah.martinAinda não há avaliações
- MOH Laboratory Requisition PDFDocumento1 páginaMOH Laboratory Requisition PDFeadmitAinda não há avaliações
- Matthew J. Friedman (Editor), Paula P. Schnurr (Editor), Terence M. Keane (Editor), Chadi Abdallah (Editor), Garrett B. Aikens (Editor) - Handbook of PTSD - Science and Practice-Guilford Press (2021)Documento691 páginasMatthew J. Friedman (Editor), Paula P. Schnurr (Editor), Terence M. Keane (Editor), Chadi Abdallah (Editor), Garrett B. Aikens (Editor) - Handbook of PTSD - Science and Practice-Guilford Press (2021)CESAR DARIO FALCON LIZANO100% (8)
- Scrotal HerniaDocumento9 páginasScrotal HerniaReymart BolagaoAinda não há avaliações
- Hpex 357 Midterm ReviewDocumento11 páginasHpex 357 Midterm ReviewJoanna RiveraAinda não há avaliações
- Scored Patient Generated Subjective Global Assessment PG SGA PDFDocumento2 páginasScored Patient Generated Subjective Global Assessment PG SGA PDFOrlea Francisco-Sisio100% (1)
- Understanding The Self - Physical & Sexual SelfDocumento5 páginasUnderstanding The Self - Physical & Sexual SelfSharmaine BeranAinda não há avaliações
- MCN-OB Questions and RationalesDocumento23 páginasMCN-OB Questions and RationalesRI NA100% (3)
- Case Study,,,,,,pneumoniaDocumento52 páginasCase Study,,,,,,pneumoniaJaillah Reigne Cura0% (1)
- Antimalarial DrugsDocumento6 páginasAntimalarial Drugsrajendra kumar SwamiAinda não há avaliações
- GoitreDocumento20 páginasGoitreSuma100% (1)
- Rayneilda Eleana Siew MLT U29 Unit Makmal Patologi Hospital Nukleus WP LabuanDocumento17 páginasRayneilda Eleana Siew MLT U29 Unit Makmal Patologi Hospital Nukleus WP LabuanValentine Brokenz Saintz100% (1)
- Case Histroy Form by Dr. Jawahar ShahDocumento21 páginasCase Histroy Form by Dr. Jawahar ShahShubhanshi BhasinAinda não há avaliações
- Ingested PoisonsDocumento39 páginasIngested PoisonsCristina L. JaysonAinda não há avaliações
- Chapter 1Documento7 páginasChapter 1Michael Charles James GingcoAinda não há avaliações
- Nursing Care of The High-Risk Postpartum ClientDocumento56 páginasNursing Care of The High-Risk Postpartum ClientMarrianne Manulat Baco100% (2)
- Endocrine System: Dr. Dedi Ardinata, M.Kes Physiology Department Medical School of University Sumatera UtaraDocumento94 páginasEndocrine System: Dr. Dedi Ardinata, M.Kes Physiology Department Medical School of University Sumatera UtaraAdryansyah ChaniagoAinda não há avaliações
- Case Presentation On GbsDocumento23 páginasCase Presentation On GbsRucHi ShArmaAinda não há avaliações
- DNHE Assignments Jan - July 2021 (English)Documento9 páginasDNHE Assignments Jan - July 2021 (English)Madhu SinghAinda não há avaliações
- Aggression and AbuseDocumento12 páginasAggression and AbuseAdede SadarakaAinda não há avaliações
- Case Study On End Stage Renal FailureDocumento19 páginasCase Study On End Stage Renal Failurelenecarglbn100% (1)
- Bennet - What Jung Really Said (1983)Documento195 páginasBennet - What Jung Really Said (1983)Sunflower0% (1)
- Patho Questions and AnswersDocumento8 páginasPatho Questions and AnswersAbdullah Kadir Hillaluddin100% (3)
- Venesection: Phlebotomy orDocumento20 páginasVenesection: Phlebotomy orVera June RañesesAinda não há avaliações