Você também pode gostar
- MD2 Pathology May 2018Documento13 páginasMD2 Pathology May 2018vicbart11Ainda não há avaliações
- Adrenal Cortex DR - GomezDocumento13 páginasAdrenal Cortex DR - Gomezvicbart11Ainda não há avaliações
- PATHO - Prelims 1.1 - The Cell As A Unit of Health & Diseases (Dela Rosa) - TRANSDocumento5 páginasPATHO - Prelims 1.1 - The Cell As A Unit of Health & Diseases (Dela Rosa) - TRANSvicbart11Ainda não há avaliações
- Blood SupplyDocumento2 páginasBlood Supplyvicbart11Ainda não há avaliações
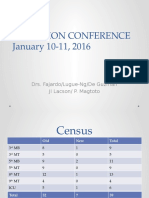
- Auf Im Adcon Jan1016-1Documento41 páginasAuf Im Adcon Jan1016-1vicbart11Ainda não há avaliações
- Physiology Feedback: Finals Sem1 Ay 2017-2018: D. Both A & B (Phospagen andDocumento4 páginasPhysiology Feedback: Finals Sem1 Ay 2017-2018: D. Both A & B (Phospagen andvicbart11Ainda não há avaliações
- Jurnal 3Documento15 páginasJurnal 3rio ramadhonaAinda não há avaliações
- Hiurationale For PTreatment of HypertensionDocumento24 páginasHiurationale For PTreatment of Hypertensionvicbart11Ainda não há avaliações
- Storage PolysaccharidesDocumento8 páginasStorage Polysaccharidesvicbart11Ainda não há avaliações
- TrematodesDocumento5 páginasTrematodesvicbart11Ainda não há avaliações
- PUBHEALTHDocumento48 páginasPUBHEALTHvicbart11Ainda não há avaliações
- Physicochemical IncompatibilitiesDocumento20 páginasPhysicochemical Incompatibilitiesvicbart11Ainda não há avaliações
- Census SurheroDocumento21 páginasCensus Surherovicbart11Ainda não há avaliações
- DSBKJDocumento13 páginasDSBKJvicbart11Ainda não há avaliações
- Blood 2Documento74 páginasBlood 2vicbart11Ainda não há avaliações
- GSJGFJ SPDocumento11 páginasGSJGFJ SPvicbart11Ainda não há avaliações
- Lectgiugdfiugsdsdkjasjure 9Documento9 páginasLectgiugdfiugsdsdkjasjure 9vicbart11Ainda não há avaliações
- Spashdvhafsdring 2013 Lecture 2fgjagfja6Documento6 páginasSpashdvhafsdring 2013 Lecture 2fgjagfja6vicbart11Ainda não há avaliações
- Lectgiugdfiugsdsdkjasjure 9Documento9 páginasLectgiugdfiugsdsdkjasjure 9vicbart11Ainda não há avaliações
- NKJDFGDocumento24 páginasNKJDFGvicbart11Ainda não há avaliações
- Storage PolysaccharidesDocumento8 páginasStorage Polysaccharidesvicbart11Ainda não há avaliações
- WATER Is The Solvent of Choice For BiologicalDocumento15 páginasWATER Is The Solvent of Choice For Biologicalvicbart11Ainda não há avaliações
- Asfldjsohspring 2013 Lecture 1hkjsgdiuaDocumento9 páginasAsfldjsohspring 2013 Lecture 1hkjsgdiuavicbart11Ainda não há avaliações
- Acid-Bases EquilibriaDocumento3 páginasAcid-Bases EquilibriacliffmusicgirlAinda não há avaliações
- Particle Size and Surface Area Are Important Parameters in The Development of A DrugDocumento8 páginasParticle Size and Surface Area Are Important Parameters in The Development of A Drugvicbart11Ainda não há avaliações
- List of Gram Positive and GramDocumento9 páginasList of Gram Positive and Gramvicbart11Ainda não há avaliações
- Angeles University Foundation Angeles University Foundation: Number of Hours Number of HoursDocumento1 páginaAngeles University Foundation Angeles University Foundation: Number of Hours Number of Hoursvicbart11Ainda não há avaliações
- Peroopidic TableDocumento2 páginasPeroopidic Tablevicbart110% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- NCCC - Melanoma Assessment and Management of Melanoma, 2015Documento886 páginasNCCC - Melanoma Assessment and Management of Melanoma, 2015Anca-Raluca PascuAinda não há avaliações
- A Dictionary For Psychotherapists PDFDocumento1.375 páginasA Dictionary For Psychotherapists PDFMonica100% (2)
- Ericksonian Hypnosis Techniques PDFDocumento2 páginasEricksonian Hypnosis Techniques PDFJakara25% (4)
- 3p7p Protocol For CosmodicDocumento3 páginas3p7p Protocol For CosmodicBacean Aurel Ioan100% (1)
- Postpartum Care: Emergency SignsDocumento13 páginasPostpartum Care: Emergency SignsJohnnette BedoniaAinda não há avaliações
- Healthy Food PDFDocumento8 páginasHealthy Food PDFnurul syafizatul shahirahAinda não há avaliações
- KKDAT Lecture, Re PNP Program Trust For Illegal DrugsDocumento43 páginasKKDAT Lecture, Re PNP Program Trust For Illegal Drugsrochelle palino85% (33)
- Steam Distilation PDFDocumento9 páginasSteam Distilation PDFAlam LazuardiAinda não há avaliações
- Child Psychiatric EmergenciesDocumento8 páginasChild Psychiatric EmergenciesDanitza YhovannaAinda não há avaliações
- Planning Physical Facilities of Hospital and Educational InstitutionDocumento5 páginasPlanning Physical Facilities of Hospital and Educational InstitutionSundaraBharathi100% (2)
- Psyc Essay Final 010420Documento2 páginasPsyc Essay Final 010420Ali HajassdolahAinda não há avaliações
- Rumah Sakit Bhakti MuliaDocumento3 páginasRumah Sakit Bhakti MuliaSarachanda SallyAinda não há avaliações
- Jordo's Beginner's Guide To Healthy and Sustainable Dieting PDFDocumento22 páginasJordo's Beginner's Guide To Healthy and Sustainable Dieting PDFSol Albi100% (2)
- HypopituitarismDocumento2 páginasHypopituitarismAnne de VeraAinda não há avaliações
- Nutritional Considerations in Geriatrics: Review ArticleDocumento4 páginasNutritional Considerations in Geriatrics: Review ArticleKrupali JainAinda não há avaliações
- Stugeron ForteDocumento4 páginasStugeron ForteJemsMei Comparativo MensuradoAinda não há avaliações
- Integrating Modern Dermatology and AyurvedaDocumento25 páginasIntegrating Modern Dermatology and AyurvedachandusgAinda não há avaliações
- Spasmophilia Comorbidity in Fibromyalgia SyndromeDocumento6 páginasSpasmophilia Comorbidity in Fibromyalgia SyndromenovywardanaAinda não há avaliações
- Strabismus and Diplopia After Refractive SurgeryDocumento5 páginasStrabismus and Diplopia After Refractive Surgeryyuda saputraAinda não há avaliações
- Interview Questions Band 5 PTDocumento7 páginasInterview Questions Band 5 PTGeorge Noorland50% (2)
- Red, Yellow and Green Flags For Low Back Pain: For Serious Underlying DiseaseDocumento1 páginaRed, Yellow and Green Flags For Low Back Pain: For Serious Underlying DiseaseShafira DianiAinda não há avaliações
- Walk in Urgent Care ServicesDocumento2 páginasWalk in Urgent Care ServicesMichel harryAinda não há avaliações
- 4 Brunnstrom ApproachDocumento18 páginas4 Brunnstrom ApproachHabibieNaufal ChannelAinda não há avaliações
- Bhasa InggrisDocumento23 páginasBhasa InggrisrinaAinda não há avaliações
- Appi Psychotherapy 20220018Documento8 páginasAppi Psychotherapy 20220018consulta.nicolaslabbeAinda não há avaliações
- Labs and Impaired Tissue...Documento40 páginasLabs and Impaired Tissue...Lea FestejoAinda não há avaliações
- Unusual Presentation of Recurrent Appendicitis - A Rare Case Report and Literature ReviewDocumento4 páginasUnusual Presentation of Recurrent Appendicitis - A Rare Case Report and Literature ReviewMirachel AugustAinda não há avaliações
- Concept of Disease 1.1 Anatomy and PhysiologyDocumento15 páginasConcept of Disease 1.1 Anatomy and PhysiologyAulia SandraAinda não há avaliações
- Clasificare Carii Dentare Otr Cariologie An IIIDocumento79 páginasClasificare Carii Dentare Otr Cariologie An IIIStefana NanuAinda não há avaliações
- Oncology Drills With Answers and RationalesDocumento41 páginasOncology Drills With Answers and RationalesCarol Kayas100% (1)