Você também pode gostar
- Bell's Palsy Pathophysiology LongDocumento4 páginasBell's Palsy Pathophysiology LongJad Paulo Gatera50% (2)
- Bell's Palsy Facial Nerve ParalysisDocumento37 páginasBell's Palsy Facial Nerve Paralysiswahyu_sitaAinda não há avaliações
- Bell's PalsyDocumento17 páginasBell's PalsyAngelie_Elvamb_8952100% (1)
- Bell''s PalsyDocumento54 páginasBell''s Palsywahyu_sitaAinda não há avaliações
- Bell's Palsy EbnDocumento48 páginasBell's Palsy EbnClara Maey GarciaAinda não há avaliações
- Benign Tumors of The StomachDocumento55 páginasBenign Tumors of The Stomachapi-19641337Ainda não há avaliações
- Gowrishankar Potturi: B.P.T, M.PT, M.I.A.P, M.I.A.C.PDocumento24 páginasGowrishankar Potturi: B.P.T, M.PT, M.I.A.P, M.I.A.C.PMuhammad Luqmanulhakim Abu Bakar100% (1)
- In General, Amputation of Limbs Is TheDocumento11 páginasIn General, Amputation of Limbs Is TheCay Sevilla100% (1)
- Neck Trauma LecDocumento49 páginasNeck Trauma Lecapi-3743483100% (2)
- Department OF Physiotherapy: Bell'S PalsyDocumento2 páginasDepartment OF Physiotherapy: Bell'S PalsybenjiAinda não há avaliações
- Acute Urinary RetentionDocumento14 páginasAcute Urinary RetentionTP RMadAinda não há avaliações
- Facial Nerve Paralysis 2Documento44 páginasFacial Nerve Paralysis 2Omowole GbengaAinda não há avaliações
- Indirect Inguinal HerniaDocumento53 páginasIndirect Inguinal HerniaYlamher Bufi ImperialAinda não há avaliações
- Inflammatory Bowel DiseaseDocumento12 páginasInflammatory Bowel DiseasemoonsoundAinda não há avaliações
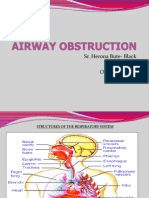
- Sr. Herona Bute- Black D.O.N.E October 7th 2011Documento35 páginasSr. Herona Bute- Black D.O.N.E October 7th 2011Jemicia AdamsAinda não há avaliações
- Seminar: Facial Nerve PalsyDocumento166 páginasSeminar: Facial Nerve PalsyShouvik ChowdhuryAinda não há avaliações
- Muscular DystrophyDocumento3 páginasMuscular Dystrophyderrickmason626Ainda não há avaliações
- Describing WoundsDocumento4 páginasDescribing WoundsDidikPrasetyoSuliAinda não há avaliações
- Diagnosis and Treatment of Otitis Media in ChildrenDocumento19 páginasDiagnosis and Treatment of Otitis Media in ChildrenreyhanrrAinda não há avaliações
- TRACTION LavlyDocumento9 páginasTRACTION Lavlylabsky_evol100% (1)
- Chapter 22 - Management of Patients With Upper Respiratory Tract Disorders (INCOMPLETEon 13)Documento16 páginasChapter 22 - Management of Patients With Upper Respiratory Tract Disorders (INCOMPLETEon 13)Mary Singleton100% (1)
- TractionsDocumento16 páginasTractionsJasmin Jacob100% (1)
- OsteoarthritisDocumento0 páginaOsteoarthritisYunita MarwahAinda não há avaliações
- OSTEOARTHRITISDocumento4 páginasOSTEOARTHRITISapi-3822433100% (2)
- Symptoms, Causes and Treatment of Inflammatory Bowel Disease (IBDDocumento24 páginasSymptoms, Causes and Treatment of Inflammatory Bowel Disease (IBDmydewyboyAinda não há avaliações
- COPD Make-Up Assignment FINALDocumento9 páginasCOPD Make-Up Assignment FINALlmstar980% (1)
- Immunisation ChartDocumento20 páginasImmunisation ChartNuha ZhafirahAinda não há avaliações
- Peripheral Vascular DiseaseDocumento36 páginasPeripheral Vascular DiseaseKeishla M Rios CardonaAinda não há avaliações
- Performance Checklist On Cranial Nerve AssessmentDocumento3 páginasPerformance Checklist On Cranial Nerve AssessmentSolsona Natl HS Maananteng100% (1)
- Pathophysiology of Ureteral CalculiDocumento14 páginasPathophysiology of Ureteral CalculiEdmel Pamplona DuquesaAinda não há avaliações
- Chapter 02 Short Case On Parotid SwellingDocumento6 páginasChapter 02 Short Case On Parotid SwellingMonir Hossain Reza0% (1)
- Staghorn CalculiDocumento60 páginasStaghorn CalculiEndang Yulia Angraini100% (1)
- Anaphylactic ShockDocumento24 páginasAnaphylactic ShockEve Megan AbingAinda não há avaliações
- Case 5 - Pancreatitis-1Documento4 páginasCase 5 - Pancreatitis-1ngAinda não há avaliações
- Bacterial MeningitisDocumento43 páginasBacterial MeningitisAthit Wutthisanwatthana100% (1)
- Nursing Management of SeizuresDocumento7 páginasNursing Management of SeizuresEcaroh Hew SmailliwAinda não há avaliações
- Emergency Drugs / Orthodontic Courses by Indian Dental AcademyDocumento74 páginasEmergency Drugs / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Perichondritis PinnaDocumento2 páginasPerichondritis PinnaAnish RajAinda não há avaliações
- Bells PalsyDocumento18 páginasBells PalsyDr AnandAinda não há avaliações
- Facial PalsyDocumento42 páginasFacial PalsyAndrew Sabastian Geraldyno PaagoAinda não há avaliações
- Open Reduction Internal Fixation RifDocumento16 páginasOpen Reduction Internal Fixation RifNurul Hidayah100% (2)
- Opioid Analgesics: © 2012 The Mcgraw-Hill Companies, Inc. All Rights ReservedDocumento47 páginasOpioid Analgesics: © 2012 The Mcgraw-Hill Companies, Inc. All Rights ReservedSana Javed100% (1)
- OSTEOARTHRITISDocumento53 páginasOSTEOARTHRITISRiza Umami100% (1)
- Clinical Practice Guidelines: Chronic Suppurative Otitis Media in AdultsDocumento28 páginasClinical Practice Guidelines: Chronic Suppurative Otitis Media in Adultsnanu-jenuAinda não há avaliações
- Elderly Nursing Case StudyDocumento13 páginasElderly Nursing Case StudysatraAinda não há avaliações
- ThyrotoxicosisDocumento42 páginasThyrotoxicosisShaw Khan100% (7)
- Emergency Drugs and Its UsesDocumento80 páginasEmergency Drugs and Its Usesjigar21Ainda não há avaliações
- Bells PalsyDocumento34 páginasBells Palsymandut987Ainda não há avaliações
- Bells PalsyDocumento33 páginasBells PalsyzzakieAinda não há avaliações
- Bell Palsy: Nelson Textbook of Pediatrics 19 EditionDocumento11 páginasBell Palsy: Nelson Textbook of Pediatrics 19 EditionTommy YauAinda não há avaliações
- Cervoni2017 4Documento5 páginasCervoni2017 4ekanovicaAinda não há avaliações
- Facial Nerve Palsy: Dr. Saud AlromaihDocumento74 páginasFacial Nerve Palsy: Dr. Saud AlromaihChandra ManapaAinda não há avaliações
- HYDROCEPHALUSDocumento63 páginasHYDROCEPHALUSJohnsatish Rudrapogu50% (2)
- 11.kuliah International 2009Documento35 páginas11.kuliah International 2009Magfira Al HabsyiAinda não há avaliações
- Facial Palsy: Lecturer: Vivien PuspitasariDocumento44 páginasFacial Palsy: Lecturer: Vivien PuspitasariCandice LavigneAinda não há avaliações
- Peripheral Neuropathy: Neurology Rotation Lecture SeriesDocumento9 páginasPeripheral Neuropathy: Neurology Rotation Lecture SeriesFandi Dwi CahyandiAinda não há avaliações
- Facial Nerve Palsy Diagnosis and TreatmentDocumento3 páginasFacial Nerve Palsy Diagnosis and TreatmentGayle VillarizaAinda não há avaliações
- PediatricsDocumento38 páginasPediatricskhanAinda não há avaliações
- Demyelinating DiseaseDocumento42 páginasDemyelinating Diseasemirabel IvanaliAinda não há avaliações
- Guillain Barre Syndrome (GBS)Documento29 páginasGuillain Barre Syndrome (GBS)Sujit KoiralaAinda não há avaliações
- Cesarean Scar Pregnancy - Tertiary-Centre Experience - MedCrave Online - WebarchiveDocumento13 páginasCesarean Scar Pregnancy - Tertiary-Centre Experience - MedCrave Online - WebarchiveJoyceAinda não há avaliações
- Methotrexate in Management of Morbidly Adherent Placenta at Latifa Hospital, DHA, Dubai, UAE. - Case .WebarchiveDocumento14 páginasMethotrexate in Management of Morbidly Adherent Placenta at Latifa Hospital, DHA, Dubai, UAE. - Case .WebarchiveJoyceAinda não há avaliações
- Leaflet DMDocumento2 páginasLeaflet DMJoyceAinda não há avaliações
- Daftar Pustaka 2Documento3 páginasDaftar Pustaka 2Muhammad Hafidz AzhariAinda não há avaliações
- 7 - Nursing Service Floating and Pull OutDocumento4 páginas7 - Nursing Service Floating and Pull Outakositabon100% (3)
- Procedures in Obstetrics and Gynaecology TextbookDocumento272 páginasProcedures in Obstetrics and Gynaecology TextbookPriyaAinda não há avaliações
- Clinical Practice Guidelines For Rest OrthosisDocumento8 páginasClinical Practice Guidelines For Rest OrthosisJavier HonoldAinda não há avaliações
- 1 - Indocyanine Green-Enhanced Fluorescence To Assess BowelDocumento7 páginas1 - Indocyanine Green-Enhanced Fluorescence To Assess BowelIcaro DanielAinda não há avaliações
- Nice Neotech - Accessories - 20Documento1 páginaNice Neotech - Accessories - 20David Gnana DuraiAinda não há avaliações
- Impaired Gas Exchange NCPDocumento1 páginaImpaired Gas Exchange NCPCj AlconabaAinda não há avaliações
- Thyroid Diseases in Pregnancy PMK HandoutDocumento12 páginasThyroid Diseases in Pregnancy PMK HandoutWikrom Keng WromKiAinda não há avaliações
- Introduction To Emergency Medical Services (EMS)Documento17 páginasIntroduction To Emergency Medical Services (EMS)ishak1863Ainda não há avaliações
- Attesta™ DR Mri Surescan™ Atdr01: Dual Chamber Rate Responsive Pacemaker (DDDR)Documento42 páginasAttesta™ DR Mri Surescan™ Atdr01: Dual Chamber Rate Responsive Pacemaker (DDDR)mytake100Ainda não há avaliações
- Definition and Characteristics of AntibioticsDocumento4 páginasDefinition and Characteristics of AntibioticsfirozbangladeshAinda não há avaliações
- Overweight, Hypertension and Heart Disease ClassificationsDocumento4 páginasOverweight, Hypertension and Heart Disease Classificationsjagadish chandra prasadAinda não há avaliações
- Differences Between T.solium and T.saginata: Taeniasis or CysticercosisDocumento3 páginasDifferences Between T.solium and T.saginata: Taeniasis or CysticercosisVenkatapradeepAinda não há avaliações
- Indirect Digital Workflow For Virtual Cross-Mounting of Fixed Implant-Supported Prostheses To Create A 3D Virtual PatientDocumento6 páginasIndirect Digital Workflow For Virtual Cross-Mounting of Fixed Implant-Supported Prostheses To Create A 3D Virtual PatientPhanQuangHuyAinda não há avaliações
- Apl 1Documento45 páginasApl 1api-243480627Ainda não há avaliações
- Heritage Health - Pre Auth FormDocumento6 páginasHeritage Health - Pre Auth FormBOOKREADER_NOWAinda não há avaliações
- Demodex CanisDocumento19 páginasDemodex Canisapi-337841627Ainda não há avaliações
- Nursing Care PlanDocumento2 páginasNursing Care PlanJewelyn Bronda100% (2)
- 23 ENT DiordersDocumento114 páginas23 ENT Diordersmohamed shamsAinda não há avaliações
- CV Peneliti UtamaDocumento14 páginasCV Peneliti Utamabidan lidiafAinda não há avaliações
- RSP20110601Documento64 páginasRSP20110601Abhinav SinghalAinda não há avaliações
- EmekaDocumento17 páginasEmekamutiyasAinda não há avaliações
- Chapter 4 Communicable DiseaseDocumento33 páginasChapter 4 Communicable DiseaseAyro Business CenterAinda não há avaliações
- Chapter 24 - Arthritis - Osteoarthritis, Gout, & Amp Rheumatoid ArthritisDocumento23 páginasChapter 24 - Arthritis - Osteoarthritis, Gout, & Amp Rheumatoid ArthritisHarris GhifaryAinda não há avaliações
- SENCHS Joins The Philippine Dengue AwarenessDocumento3 páginasSENCHS Joins The Philippine Dengue AwarenessFhikery ArdienteAinda não há avaliações
- 2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentDocumento9 páginas2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentCharley WangAinda não há avaliações
- E202 Medical Assessment PDFDocumento1 páginaE202 Medical Assessment PDFSyahidatul Kautsar NajibAinda não há avaliações
- GERD Nursing CareDocumento9 páginasGERD Nursing CareTrisha ArizalaAinda não há avaliações
- Clinical Laboratory TransesDocumento2 páginasClinical Laboratory TransesjulianneAinda não há avaliações
- A Tertiary Health Care Centre Experience of The Impact of COVID On The Case Load in The Department of Obstetrics and Gynaecology at MGM Hospital, AurangabadDocumento4 páginasA Tertiary Health Care Centre Experience of The Impact of COVID On The Case Load in The Department of Obstetrics and Gynaecology at MGM Hospital, AurangabadInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- Corpectomy Cage Surgical TechniquesDocumento18 páginasCorpectomy Cage Surgical TechniquesJulian VargasAinda não há avaliações