Você também pode gostar
- Achilles Tendon Rupture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandAchilles Tendon Rupture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- A Simple Guide to Popliteal Muscle Tear, Diagnosis, Treatment and Related ConditionsNo EverandA Simple Guide to Popliteal Muscle Tear, Diagnosis, Treatment and Related ConditionsAinda não há avaliações
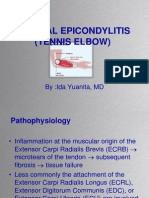
- Lateral Epicondylitis (Tennis Elbow) : By:Ida Yuanita, MDDocumento37 páginasLateral Epicondylitis (Tennis Elbow) : By:Ida Yuanita, MDAnang FajarAinda não há avaliações
- Locomotor System Study GuideDocumento80 páginasLocomotor System Study Guidemartincorbacho100% (1)
- Document 85Documento51 páginasDocument 85Shameena AnwarAinda não há avaliações
- CLOSED FRACTURE OF LEFT TIBIAL PLATEAU SCHATZKER VIDocumento41 páginasCLOSED FRACTURE OF LEFT TIBIAL PLATEAU SCHATZKER VIlukitaniningAinda não há avaliações
- Ortho Fraktur 1/3 Proximal Humerus DextraDocumento57 páginasOrtho Fraktur 1/3 Proximal Humerus DextraFian ChristoAinda não há avaliações
- Lecture 1 Patient examined method of TraumaDocumento55 páginasLecture 1 Patient examined method of TraumaTselmeg TselmegAinda não há avaliações
- Supervised Clinical Practice-III: AssignmentDocumento12 páginasSupervised Clinical Practice-III: Assignmentzainab siddiqueAinda não há avaliações
- Bilateral Knee OADocumento35 páginasBilateral Knee OAMu'iz Beatforteen50% (2)
- Case Report Rehabilitation Program in A Patient With Femoral Neck FractureDocumento26 páginasCase Report Rehabilitation Program in A Patient With Femoral Neck FractureNatalia LoredanaAinda não há avaliações
- General Format For Orthopedic AssessmentDocumento27 páginasGeneral Format For Orthopedic AssessmentMegha Patani100% (7)
- 23 Juli 2011, Ny M, Closed Multiple Fracture Distal Os Fibula Dextra + Closed Fr. Distal Os Tibia Dextra + VL, DR Iwan SPB, DR BudiDocumento35 páginas23 Juli 2011, Ny M, Closed Multiple Fracture Distal Os Fibula Dextra + Closed Fr. Distal Os Tibia Dextra + VL, DR Iwan SPB, DR BudiSteffi NatadidjajaAinda não há avaliações
- Duty Report and Patient Cases from Koja Hospital ERDocumento46 páginasDuty Report and Patient Cases from Koja Hospital ERsyazana salimAinda não há avaliações
- Tibial Plateau PowerpointDocumento28 páginasTibial Plateau PowerpointMyra MieraAinda não há avaliações
- I. Dr. Yoyos - Unstable Pelvic Fracture Jam 14Documento42 páginasI. Dr. Yoyos - Unstable Pelvic Fracture Jam 14Rsud Malinau Ppk BludAinda não há avaliações
- Hip and Buttock PainDocumento26 páginasHip and Buttock PainEdy SetiawanAinda não há avaliações
- B.an Đ T DCCT 199 T.anhDocumento7 páginasB.an Đ T DCCT 199 T.anhNhư NgọcAinda não há avaliações
- Closed Fracture TibialDocumento41 páginasClosed Fracture TibiallukitaniningAinda não há avaliações
- Tn. GiminDocumento21 páginasTn. Giminyenidwianggra sudarmajiAinda não há avaliações
- OA - Ahmad Aulia Rizaly - DR Andry Usman SpOTDocumento34 páginasOA - Ahmad Aulia Rizaly - DR Andry Usman SpOTNur Syamsiah MAinda não há avaliações
- Surgery Morning Report FracturesDocumento24 páginasSurgery Morning Report FracturesAulia Kurnia FananiAinda não há avaliações
- Shoulder pain diagnosis in diabetes patientTITLEDocumento67 páginasShoulder pain diagnosis in diabetes patientTITLEmark tAinda não há avaliações
- Closed Tibia and Fibula Fractures in 44-Year-Old Male PatientDocumento25 páginasClosed Tibia and Fibula Fractures in 44-Year-Old Male Patientleonard0% (1)
- OMM One LinersDocumento21 páginasOMM One LinersBrooklyn Boo-urns100% (1)
- 1-Year-Old Child With Left Hand Contracture After Burn InjuryDocumento45 páginas1-Year-Old Child With Left Hand Contracture After Burn InjuryPramitha Yustia100% (1)
- Long Case OrthopaedicDocumento24 páginasLong Case OrthopaedicSyimah UmarAinda não há avaliações
- Short Case II: Jufri Febrianto, MDDocumento16 páginasShort Case II: Jufri Febrianto, MDsingle_ladyAinda não há avaliações
- Treating a Closed Supracondylar Fracture of the Right FemurDocumento37 páginasTreating a Closed Supracondylar Fracture of the Right FemurSri Mahtufa Riski100% (1)
- KS LE AmputationDocumento116 páginasKS LE AmputationAstri ArfAinda não há avaliações
- Activity AssesmentDocumento4 páginasActivity AssesmentGuillana Mae CastellonAinda não há avaliações
- Knee ExaminationDocumento26 páginasKnee ExaminationMikorizaAmanitaAinda não há avaliações
- Musculoskeletal System Musculoskeletal System: A. SkeletonDocumento23 páginasMusculoskeletal System Musculoskeletal System: A. SkeletonTina TalmadgeAinda não há avaliações
- Adolescent Idiopathic Scoliosis Lenke's Classification Type 3 ADocumento49 páginasAdolescent Idiopathic Scoliosis Lenke's Classification Type 3 AAndi HumairahAinda não há avaliações
- Kelompok 2 Sken BDocumento42 páginasKelompok 2 Sken BAbu Hanan HammasinAinda não há avaliações
- Low Back Pain Lapkas 2Documento27 páginasLow Back Pain Lapkas 2rini najoanAinda não há avaliações
- Case Study On Tennis ElbowDocumento5 páginasCase Study On Tennis ElbowPriyaAinda não há avaliações
- Knee Orthopaedic TestsDocumento47 páginasKnee Orthopaedic Testsagha_sajjad90Ainda não há avaliações
- Case Report Rehabilitation Program in A Patient With A Displaced Femoral Neck FractureDocumento26 páginasCase Report Rehabilitation Program in A Patient With A Displaced Femoral Neck FractureNatalia LoredanaAinda não há avaliações
- Ankle PainnDocumento4 páginasAnkle PainngoodlucksonkiloAinda não há avaliações
- Left Achilles Tendon Rupture RepairDocumento4 páginasLeft Achilles Tendon Rupture RepairYoAinda não há avaliações
- 02.elbow PainDocumento62 páginas02.elbow PainKhushboo IkramAinda não há avaliações
- Case Presentation: HistoryDocumento45 páginasCase Presentation: HistorySaya MenangAinda não há avaliações
- Colles FractureDocumento89 páginasColles Fracturenur syafiqah kamaruzaman100% (1)
- DD Case Report Elbow DislocationDocumento33 páginasDD Case Report Elbow DislocationKurniawan Nur IhsanAinda não há avaliações
- Colles's Fracture: B (Hons.) PhysiotherapyDocumento36 páginasColles's Fracture: B (Hons.) PhysiotherapySafwan Idham RamlanAinda não há avaliações
- ER Report: 4 Patients with Orthopedic InjuriesDocumento49 páginasER Report: 4 Patients with Orthopedic InjuriesJati NugrohoAinda não há avaliações
- Climbing Injuries Prevention GuideDocumento18 páginasClimbing Injuries Prevention GuideDaniel SloskyAinda não há avaliações
- Emergency Report: RSO Prof. Dr. R. Soeharso Surakarta, Saturday, December 15 2017Documento54 páginasEmergency Report: RSO Prof. Dr. R. Soeharso Surakarta, Saturday, December 15 2017Hanif Andhika WardhanaAinda não há avaliações
- The Examination of The Knee - 040716Documento35 páginasThe Examination of The Knee - 040716Mufidah FidaAinda não há avaliações
- CASE REPORT NONUNION FEMURDocumento25 páginasCASE REPORT NONUNION FEMURnursyahilaAinda não há avaliações
- Fascial Distortion Model - Vol.4Documento76 páginasFascial Distortion Model - Vol.4Magno FilhoAinda não há avaliações
- UMS Orthopedic Short Cases Records 1st EditionDocumento15 páginasUMS Orthopedic Short Cases Records 1st EditionHayati Nasir100% (2)
- Final-Cases-5 1 09Documento80 páginasFinal-Cases-5 1 09tatig1130Ainda não há avaliações
- Artigo - JoelhoDocumento4 páginasArtigo - JoelhoizabellegoesAinda não há avaliações
- Thoracal Fracture of The SpineDocumento32 páginasThoracal Fracture of The Spinefaranur sabudinAinda não há avaliações
- Slide 1: "Open Fracture 1/3 Distal Tibia and Fibula Sinistra"Documento33 páginasSlide 1: "Open Fracture 1/3 Distal Tibia and Fibula Sinistra"Farizka Dwinda HAinda não há avaliações
- 2 Acute Shoulder Pain Diagnosis and ManagementDocumento42 páginas2 Acute Shoulder Pain Diagnosis and Managementmk78_inAinda não há avaliações
- Lapjag 11 Oktober 2019Documento41 páginasLapjag 11 Oktober 2019Martha SimonaAinda não há avaliações
- Nur Zahiera BT Muhamad Najib 030.08.298Documento46 páginasNur Zahiera BT Muhamad Najib 030.08.298Zahiera NajibAinda não há avaliações
- Glaukoma: Agustian Deny I11109090Documento59 páginasGlaukoma: Agustian Deny I11109090Agustian DenyAinda não há avaliações
- Orthopaedic ReferatDocumento23 páginasOrthopaedic ReferatAgustian DenyAinda não há avaliações
- Epidemiological Impact of A Genital Herpes Type 2 Vaccine For Young FemalesDocumento22 páginasEpidemiological Impact of A Genital Herpes Type 2 Vaccine For Young FemalesAgustian DenyAinda não há avaliações
- MR 17 Des 2015Documento13 páginasMR 17 Des 2015Agustian DenyAinda não há avaliações
- PR JurnalDocumento1 páginaPR JurnalAgustian DenyAinda não há avaliações
- MR 10 Jan 2016Documento43 páginasMR 10 Jan 2016Agustian DenyAinda não há avaliações
- Orthopaedic ReferatDocumento23 páginasOrthopaedic ReferatAgustian DenyAinda não há avaliações
- Orthopaedic ReferatDocumento23 páginasOrthopaedic ReferatAgustian DenyAinda não há avaliações
- MR 6 Jan 2016Documento48 páginasMR 6 Jan 2016Agustian DenyAinda não há avaliações
- MR 6 Jan 2016Documento48 páginasMR 6 Jan 2016Agustian DenyAinda não há avaliações
- Presentasi Jurnal 2Documento20 páginasPresentasi Jurnal 2Agustian DenyAinda não há avaliações
- Hyatt Amritsar showcases Chinese and Thai cuisineDocumento1 páginaHyatt Amritsar showcases Chinese and Thai cuisineAnmol MehanAinda não há avaliações
- Tata AIA Life Insurance Fortune Guarantee Plus Savings PlanDocumento13 páginasTata AIA Life Insurance Fortune Guarantee Plus Savings PlanAkshay SaxenaAinda não há avaliações
- Unit 4 BacteriologyDocumento51 páginasUnit 4 BacteriologySharmila LamisharAinda não há avaliações
- Bailey SafeMedPharmacyTechnicianDocumento10 páginasBailey SafeMedPharmacyTechnicianRazak AbdullahAinda não há avaliações
- Principles of Health AdminDocumento42 páginasPrinciples of Health AdminAnne BattulayanAinda não há avaliações
- GRADE 5 - WEEK 6 Catch UpDocumento8 páginasGRADE 5 - WEEK 6 Catch Upbutchabdon1992Ainda não há avaliações
- MRNA Vaccines - Day - 04.14.20 PDFDocumento259 páginasMRNA Vaccines - Day - 04.14.20 PDFTammy G100% (1)
- Experiment 5 EDTA Titration: Calcium in Calcium Supplements: Student HandoutDocumento6 páginasExperiment 5 EDTA Titration: Calcium in Calcium Supplements: Student HandoutIbad MuhammedAinda não há avaliações
- High Yield Surgery Compatible VersionDocumento77 páginasHigh Yield Surgery Compatible Version17kimpAinda não há avaliações
- Water QualityDocumento41 páginasWater QualityPaschal MazikuAinda não há avaliações
- Annual Report 2013-14Documento198 páginasAnnual Report 2013-14shahabAinda não há avaliações
- Marijuana Fact SheetDocumento1 páginaMarijuana Fact Sheetapi-355176759Ainda não há avaliações
- Pq-Unocal Csms '03Documento15 páginasPq-Unocal Csms '03Ismail Hamzah Azmatkhan Al-husainiAinda não há avaliações
- Mozart, Beethoven, Yesudas Effect Class 2Documento12 páginasMozart, Beethoven, Yesudas Effect Class 2Dr Suvarna NalapatAinda não há avaliações
- Vanessa Tarot BookletDocumento36 páginasVanessa Tarot BookletClassic Bobby100% (2)
- Wound HealingDocumento44 páginasWound HealingSorin Niky MocanuAinda não há avaliações
- Acy 087Documento14 páginasAcy 087johnsmithdosAinda não há avaliações
- New Applications August 2022Documento70 páginasNew Applications August 2022rahul kakapuriAinda não há avaliações
- Acd Iam 05 ImatDocumento2 páginasAcd Iam 05 Imatnjk realty100% (1)
- Quality Assurance in Medical LaboratoriesDocumento69 páginasQuality Assurance in Medical Laboratories"DocAxi" Maximo B Axibal Jr MD FPSP100% (1)
- Fire Safety Fundamentals and Fire Extinguisher ClassificationsDocumento3 páginasFire Safety Fundamentals and Fire Extinguisher ClassificationsGangapuram SrikanthAinda não há avaliações
- Middle Childhood Physical Development (6-11 YearsDocumento13 páginasMiddle Childhood Physical Development (6-11 YearsAngela YlaganAinda não há avaliações
- ACTION PLAN FOR JUVENILE PRISONERS IN ILOILO CITYDocumento22 páginasACTION PLAN FOR JUVENILE PRISONERS IN ILOILO CITYJohn Christian LopezAinda não há avaliações
- International Congress 1263Documento12 páginasInternational Congress 1263AksMastAinda não há avaliações
- Model Testimi Në Lëndën Gjuha Angleze, Klasa e 9, Model 1 PDFDocumento6 páginasModel Testimi Në Lëndën Gjuha Angleze, Klasa e 9, Model 1 PDFndojafernandagmail.comAinda não há avaliações
- OSHS LegislationsDocumento59 páginasOSHS LegislationsAlvin DeliroAinda não há avaliações
- Seasonality of Hepatitis ADocumento5 páginasSeasonality of Hepatitis AHaydas ChannelAinda não há avaliações
- Effect of Smoking On HalitosisDocumento5 páginasEffect of Smoking On HalitosisMaria JabbarAinda não há avaliações
- 1 s2.0 S2772569323000026 MainDocumento8 páginas1 s2.0 S2772569323000026 MainAditya RizkyAinda não há avaliações
- Occurrence and Health Risk Assessment of Pharmaceutical and Personal Care Products (PPCPS) in Tap Water of ShanghaiDocumento8 páginasOccurrence and Health Risk Assessment of Pharmaceutical and Personal Care Products (PPCPS) in Tap Water of ShanghaiTiago TorresAinda não há avaliações