Você também pode gostar
- Module Opthalmology Corneal Ulcer: Group 7 Wulan-Fadzely-Arif Amri-Safuan Arif-Nadiah-Insyira-Fatimah-Andi AbsharinaDocumento19 páginasModule Opthalmology Corneal Ulcer: Group 7 Wulan-Fadzely-Arif Amri-Safuan Arif-Nadiah-Insyira-Fatimah-Andi Absharinaarifamri92Ainda não há avaliações
- Jurding Otitis Eksterna MalignaDocumento19 páginasJurding Otitis Eksterna MalignabucexAinda não há avaliações
- Blood Supply of Brain and Spinal Cord: W Prasasti Mutiadesi, DR., M. BiomedDocumento26 páginasBlood Supply of Brain and Spinal Cord: W Prasasti Mutiadesi, DR., M. Biomedhelda dwianaAinda não há avaliações
- Kelimpahan Dan Pola Pertumbuhan Kepiting Bakau ScyDocumento8 páginasKelimpahan Dan Pola Pertumbuhan Kepiting Bakau ScyNelsi Antonius KalaAinda não há avaliações
- Morning Report CKDDocumento20 páginasMorning Report CKDjoe joeAinda não há avaliações
- Hanifin and Rajka Diagnostic Criteria For Atopic DermatitisDocumento3 páginasHanifin and Rajka Diagnostic Criteria For Atopic DermatitisAlief LeisyahAinda não há avaliações
- Pediatric Assessment TriangleDocumento13 páginasPediatric Assessment TriangleShinta NareswariAinda não há avaliações
- Direct and Indirect FinalDocumento31 páginasDirect and Indirect Finalmeenali karnAinda não há avaliações
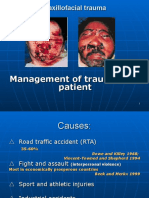
- Primary Management of Maxillofacial TraumaDocumento34 páginasPrimary Management of Maxillofacial TraumafitsumAinda não há avaliações
- Osteoartritis: Dr. Dewi Nur Fiana.,Sp - KFRDocumento28 páginasOsteoartritis: Dr. Dewi Nur Fiana.,Sp - KFRgita cahayaAinda não há avaliações
- Skull Cervical X-RayDocumento15 páginasSkull Cervical X-RayPuji Yunisyah RahayuAinda não há avaliações
- Sach IELTS 1 - Reading - HomewworkDocumento200 páginasSach IELTS 1 - Reading - Homewworkthangphi1995Ainda não há avaliações
- Retinopati DiabetikDocumento5 páginasRetinopati DiabetikMuhammad Afriadi HamdanAinda não há avaliações
- Resep THT PDFDocumento2 páginasResep THT PDFlaksonoAinda não há avaliações
- COMPASS - S&E Critical Element: Beri Tanda "X" Pada Jawaban Yang Anda Anggap BenarDocumento1 páginaCOMPASS - S&E Critical Element: Beri Tanda "X" Pada Jawaban Yang Anda Anggap BenarDidik Tri WahyudiAinda não há avaliações
- Dr. Ni Nyoman Margiani, Sprad Bagian Radiologi FK Unud/Rsup Sanglah DenpasarDocumento67 páginasDr. Ni Nyoman Margiani, Sprad Bagian Radiologi FK Unud/Rsup Sanglah DenpasarGabrielleFelindaArianiAinda não há avaliações
- Acute Scrotum 231016 PDFDocumento50 páginasAcute Scrotum 231016 PDFDany Dias100% (1)
- Subluksasi LensaDocumento12 páginasSubluksasi LensaDede GunawanAinda não há avaliações
- AntibiotikDocumento2 páginasAntibiotikTimothy OlsonAinda não há avaliações
- Radiologi ILO Terbaru (PIPKRA 2011)Documento47 páginasRadiologi ILO Terbaru (PIPKRA 2011)elsaAinda não há avaliações
- Boys Chart Arm Circumference For Age3 Months To 5 Years (Percentiles)Documento1 páginaBoys Chart Arm Circumference For Age3 Months To 5 Years (Percentiles)Rahmawati Nur AzizahAinda não há avaliações
- Lapkas 4 - Pneumonia Susp. Covid 19-Fenda KhafidhotentyDocumento17 páginasLapkas 4 - Pneumonia Susp. Covid 19-Fenda KhafidhotentydianarahimmAinda não há avaliações
- Systemic Lupus Erythematosus: Pathogenesis and Clinical FeaturesDocumento30 páginasSystemic Lupus Erythematosus: Pathogenesis and Clinical FeaturesOrion JohnAinda não há avaliações
- Referat - Trauma OculiDocumento22 páginasReferat - Trauma OculiBesseMarwah AgusHusainAinda não há avaliações
- BronkiektasisDocumento7 páginasBronkiektasisirenaAinda não há avaliações
- Intubasi Endoktrakheal 2020Documento53 páginasIntubasi Endoktrakheal 2020Octa VianiAinda não há avaliações
- Kompre Poli MataDocumento312 páginasKompre Poli MataRizaldyYogaPanduPerdanaAinda não há avaliações
- Refleksi Kasus: Tonsilitis KronisDocumento30 páginasRefleksi Kasus: Tonsilitis KronisayurahimahAinda não há avaliações
- Peran Tes Elektroakustik Imitans Di Bidang Audiologi - Prof Jenny BashiruddinDocumento29 páginasPeran Tes Elektroakustik Imitans Di Bidang Audiologi - Prof Jenny BashiruddinekaAinda não há avaliações
- Larynx InfectionsDocumento28 páginasLarynx InfectionsMuskan GogiaAinda não há avaliações
- 2 DHF InternaDocumento59 páginas2 DHF Internasaladass 2Ainda não há avaliações
- CRS SolDocumento25 páginasCRS SolDiga Ana RusfiAinda não há avaliações
- Karakteristik Klinis Dan Hasil Implantasi Lensa Intra Okular Iris Claw Pada Kasus Afakia Di Rumah Sakit Mata Cicendo - Azalia LatuasanDocumento10 páginasKarakteristik Klinis Dan Hasil Implantasi Lensa Intra Okular Iris Claw Pada Kasus Afakia Di Rumah Sakit Mata Cicendo - Azalia Latuasanwasobiru isbiruAinda não há avaliações
- Kista EndometriosisDocumento56 páginasKista EndometriosisdavinsetiamanahAinda não há avaliações
- LPRDocumento30 páginasLPRLiza HutahaeanAinda não há avaliações
- newHIBIKI Price List 2022Documento12 páginasnewHIBIKI Price List 2022johanesAinda não há avaliações
- ILMN Pricing Guide 2324Documento6 páginasILMN Pricing Guide 2324wirya designprintingAinda não há avaliações
- Care Grup UNAI Semester Genap 2020Documento55 páginasCare Grup UNAI Semester Genap 2020NaniAinda não há avaliações
- Roy ReferatDocumento8 páginasRoy ReferatFadel Aneuk NanggroeAinda não há avaliações
- Fraktur Dan Infeksi TulangDocumento25 páginasFraktur Dan Infeksi TulangAnonymous HAbhRTs2TfAinda não há avaliações
- Operasi Monokular Recess Resect Dengan Teknik: Hangback Pada Exotropia Deviasi BesarDocumento10 páginasOperasi Monokular Recess Resect Dengan Teknik: Hangback Pada Exotropia Deviasi BesarBlack Clover IdAinda não há avaliações
- Kaplan, Sadock, Grebb. 1997. Sinopsis Psikiatri Ilmu Pengetahuan Perilaku Psikiatri Klinis Jilid Satu. Jakarta: Binarupa AksaraDocumento2 páginasKaplan, Sadock, Grebb. 1997. Sinopsis Psikiatri Ilmu Pengetahuan Perilaku Psikiatri Klinis Jilid Satu. Jakarta: Binarupa AksaraLordeAinda não há avaliações
- Death Case Dr. MeikoDocumento49 páginasDeath Case Dr. MeikoMohamad ZulfikarAinda não há avaliações
- Lamp.2 Sop Evakuasi MedisDocumento2 páginasLamp.2 Sop Evakuasi MedisUci HasbullahAinda não há avaliações
- Mata Merah, Visus Normal - 1Documento51 páginasMata Merah, Visus Normal - 1nashqonashAinda não há avaliações
- Referat Kandidosis Kutis - Dhira Dan A. Fari-70700120034 Dan 038Documento14 páginasReferat Kandidosis Kutis - Dhira Dan A. Fari-70700120034 Dan 038Ahmad Fari Arief LopaAinda não há avaliações
- Gambar UlkusDocumento5 páginasGambar UlkusMaria Margareta HutajuluAinda não há avaliações
- Anatomi JantungDocumento2 páginasAnatomi JantungAuliya NaimahAinda não há avaliações
- Eritroderma - Bolognia 4th EditionDocumento15 páginasEritroderma - Bolognia 4th EditionAisyahAinda não há avaliações
- Fix Case Report TifoidDocumento24 páginasFix Case Report Tifoidanggun nur auliaAinda não há avaliações
- Expanded Dengue Syndrome: Zukmianty SuaibDocumento45 páginasExpanded Dengue Syndrome: Zukmianty SuaibclaraAinda não há avaliações
- AspergillomaDocumento20 páginasAspergillomaFatur ReyhanAinda não há avaliações
- Guideline - Training New Trainer ISMKI 2016Documento18 páginasGuideline - Training New Trainer ISMKI 2016Dhery Dev WhitterAinda não há avaliações
- Status Epileptikus Morning ReportDocumento16 páginasStatus Epileptikus Morning Reportlie antoAinda não há avaliações
- Leaflet DM Puasa Rev 5Documento2 páginasLeaflet DM Puasa Rev 5Fitria SlameutAinda não há avaliações
- Cogan-Reese Syndrome - A Rare Case of Unilateral GlaucomaDocumento8 páginasCogan-Reese Syndrome - A Rare Case of Unilateral GlaucomaDr. Abhishek OnkarAinda não há avaliações
- OPHTHA Case Report Diabetic RetinopathyDocumento51 páginasOPHTHA Case Report Diabetic RetinopathyJessa MeaAinda não há avaliações
- Panuveitis With Disc Edema After Dengue Fever: A Rare PresentationDocumento3 páginasPanuveitis With Disc Edema After Dengue Fever: A Rare PresentationRio AlexanderAinda não há avaliações
- Anatomi Dan Fisiologi KorneaDocumento133 páginasAnatomi Dan Fisiologi KorneaAriyanie NurtaniaAinda não há avaliações
- Presentasi Kasus Glaukoma AkutDocumento24 páginasPresentasi Kasus Glaukoma AkutHendrawan Ariwibowo100% (1)
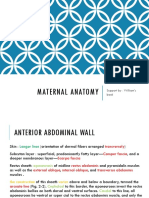
- Chapter 2 Maternal Anatomy WilliamsDocumento60 páginasChapter 2 Maternal Anatomy WilliamsDiskaAstariniAinda não há avaliações
- Normal Puerperium & Lactation Dr. Renu SinghDocumento29 páginasNormal Puerperium & Lactation Dr. Renu SinghDiskaAstariniAinda não há avaliações
- Physiologicalchangesduringpregnancy 120719105010 Phpapp02Documento36 páginasPhysiologicalchangesduringpregnancy 120719105010 Phpapp02DiskaAstariniAinda não há avaliações
- Keganasan Plasenta AkretaDocumento13 páginasKeganasan Plasenta AkretaDiskaAstariniAinda não há avaliações
- Chapter 3 Genitourinary AbnormalityDocumento20 páginasChapter 3 Genitourinary AbnormalityDiskaAstariniAinda não há avaliações
- Presentation 1Documento2 páginasPresentation 1DiskaAstariniAinda não há avaliações
- Lisa Payne - Group Leader: Sharron Beasley Venessa Escobar Kristy Fendley Brenda Jackson Vanessa Martin Natasha VillarsDocumento19 páginasLisa Payne - Group Leader: Sharron Beasley Venessa Escobar Kristy Fendley Brenda Jackson Vanessa Martin Natasha VillarsDiskaAstariniAinda não há avaliações
- Chapter 4 Maternal PhysiologyDocumento3 páginasChapter 4 Maternal PhysiologyDiskaAstariniAinda não há avaliações
- Chapter 4 Maternal PhysiologyDocumento3 páginasChapter 4 Maternal PhysiologyDiskaAstariniAinda não há avaliações
- Leukocoria 2016Documento35 páginasLeukocoria 2016DiskaAstarini100% (1)
- Chapter 3 Genitourinary AbnormalityDocumento20 páginasChapter 3 Genitourinary AbnormalityDiskaAstariniAinda não há avaliações
- LensDocumento1 páginaLensDiskaAstariniAinda não há avaliações
- Healing of CorneaDocumento10 páginasHealing of CorneaDiskaAstariniAinda não há avaliações
- Relative Afferent Pupillary DefectDocumento11 páginasRelative Afferent Pupillary DefectDiskaAstariniAinda não há avaliações
- Document (3) GDocumento5 páginasDocument (3) GDiskaAstariniAinda não há avaliações
- Leukocoria 2016fixDocumento37 páginasLeukocoria 2016fixDiskaAstariniAinda não há avaliações
- Red Eye With Normal VisionDocumento58 páginasRed Eye With Normal VisionDiskaAstariniAinda não há avaliações
- Jurnal Reading IpdDocumento12 páginasJurnal Reading IpdDiskaAstariniAinda não há avaliações
- Radiology of The Respiratory SystemDocumento184 páginasRadiology of The Respiratory SystemDiskaAstariniAinda não há avaliações
- My Dissa PresentDocumento39 páginasMy Dissa PresentDiskaAstariniAinda não há avaliações
- Case OculiDocumento25 páginasCase OculiDiskaAstariniAinda não há avaliações
- Chronic Visual LossDocumento8 páginasChronic Visual LossDiskaAstariniAinda não há avaliações
- Case OculiDocumento25 páginasCase OculiDiskaAstariniAinda não há avaliações
- Jured Bedah SarapDocumento11 páginasJured Bedah SarapDiskaAstariniAinda não há avaliações
- Kcal #ColorDocumento12 páginasKcal #ColorRinaldhiHarifPunandityaAinda não há avaliações
- CO PY: Shutter ButtonDocumento1 páginaCO PY: Shutter ButtonSonora147Ainda não há avaliações
- Visual Field InterpretationDocumento11 páginasVisual Field Interpretationhameed28885Ainda não há avaliações
- Vizio E701i-A3 CNET Review Calibration ResultsDocumento7 páginasVizio E701i-A3 CNET Review Calibration ResultsDavid KatzmaierAinda não há avaliações
- July-2021 Finished Chemicals StockDocumento2 páginasJuly-2021 Finished Chemicals StocktianAinda não há avaliações
- Daftar Kalibrasi Alat RSKM ProvsumselDocumento2 páginasDaftar Kalibrasi Alat RSKM ProvsumselNiko AndreanAinda não há avaliações
- Jazzie Joyce Laceda: Macro LensesDocumento2 páginasJazzie Joyce Laceda: Macro LensesPotpot LacedaAinda não há avaliações
- Shades of White: Rendering in WatercolorDocumento4 páginasShades of White: Rendering in WatercolorMichael Reardon100% (4)
- Tahapan FotogrametriDocumento3 páginasTahapan Fotogrametriadnan yusufAinda não há avaliações
- 4 115153222871556219 PDFDocumento392 páginas4 115153222871556219 PDFSaurabh JainAinda não há avaliações
- PhotopsinDocumento3 páginasPhotopsinandrej.gregorcicAinda não há avaliações
- 2d Art SyllabusDocumento9 páginas2d Art Syllabusapi-331571545Ainda não há avaliações
- SCIENCE 8 Q1 Module 5 Colors of LightDocumento1 páginaSCIENCE 8 Q1 Module 5 Colors of LightBENNY CALLOAinda não há avaliações
- TLE9 Module 5 6Documento37 páginasTLE9 Module 5 6Teacher EmAinda não há avaliações
- Human Eye and Colourful World (PW)Documento16 páginasHuman Eye and Colourful World (PW)Rahul ChoudharyAinda não há avaliações
- Ocular Emergencies DR Wisudawan SPM - KelaskedokteranDocumento22 páginasOcular Emergencies DR Wisudawan SPM - KelaskedokteranMonna Medani LysabellaAinda não há avaliações
- Sony F35 PDFDocumento24 páginasSony F35 PDFCode 9Ainda não há avaliações
- WindischDocumento303 páginasWindischgrininja100% (1)
- Fundus PhotoDocumento10 páginasFundus PhotoWong Jia YingAinda não há avaliações
- Lamp Digital Working 2021 EspañolDocumento491 páginasLamp Digital Working 2021 EspañolVEMATELAinda não há avaliações
- WP - 10 Tips For Aspiring PhotographersDocumento11 páginasWP - 10 Tips For Aspiring PhotographersHeliblueAinda não há avaliações
- Clinical Study On Acupuncture For Quality of Life in Patients With Age-Related Macular DegenerationDocumento5 páginasClinical Study On Acupuncture For Quality of Life in Patients With Age-Related Macular DegenerationathiaAinda não há avaliações
- Definition of Terms: Learning OutcomesDocumento8 páginasDefinition of Terms: Learning OutcomesMichelle DadiosAinda não há avaliações
- Girl-Up BrandGuidelines 0802Documento24 páginasGirl-Up BrandGuidelines 0802naveed khanAinda não há avaliações
- WLS Pro IO-Link Data Reference Guide: Instruction ManualDocumento46 páginasWLS Pro IO-Link Data Reference Guide: Instruction ManualJimyAinda não há avaliações
- Video CameraDocumento26 páginasVideo Camerasakshimann2004Ainda não há avaliações
- Graphic Design Exampleslines and ShapesDocumento15 páginasGraphic Design Exampleslines and Shapesjevieconsultaaquino2003Ainda não há avaliações
- Arts 1 Second Grading ExamDocumento10 páginasArts 1 Second Grading ExamJoniele Angelo AninAinda não há avaliações
- BTVC Series T Shape Dual-Sensor Thermal CameraDocumento3 páginasBTVC Series T Shape Dual-Sensor Thermal CameraRiyadh MirzaAinda não há avaliações
- Shekar Nethralaya: Complete Eye Care SolutionsDocumento16 páginasShekar Nethralaya: Complete Eye Care SolutionsShubham MaheshwariAinda não há avaliações