Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Development of The Mandible: Dr. Kemer KDocumento41 páginasDevelopment of The Mandible: Dr. Kemer KLintoAinda não há avaliações
- Cn7 Palsy (Bells Palsy)Documento5 páginasCn7 Palsy (Bells Palsy)Wande AyodeleAinda não há avaliações
- Nodul Tiroidian Engleza PPT 2016Documento36 páginasNodul Tiroidian Engleza PPT 2016Stefi GrAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Sonography of Normal and Abnormal Thyroid and Parathyroid Glands PDFDocumento15 páginasSonography of Normal and Abnormal Thyroid and Parathyroid Glands PDFJheyson Javier Barrios PereiraAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- TireotoxicozaDocumento3 páginasTireotoxicozaDragos PopoviciAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Correlative Clinical Anatomy of The Head: Joel G. Soria, MDDocumento52 páginasCorrelative Clinical Anatomy of The Head: Joel G. Soria, MDSugeng Supoyo Pawit DigdotriratnaAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Labreportnew - 2022-12-17T172351.750Documento1 páginaLabreportnew - 2022-12-17T172351.750Himanshu MaheshwariAinda não há avaliações
- 1 SMDocumento3 páginas1 SMDea favellaAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Face SubunitsDocumento5 páginasFace SubunitsDeevish N DinakarAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Gingival Biotype Classification, Assessment, and Clinical Importance: A ReviewDocumento7 páginasGingival Biotype Classification, Assessment, and Clinical Importance: A ReviewKetherin LeeAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- HANDOUT Laryngeal-MassageDocumento7 páginasHANDOUT Laryngeal-MassageAnca OAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hematosinus RadiologiDocumento16 páginasHematosinus RadiologiAfdalAinda não há avaliações
- Patient Type: OPD: TSH Test ReportDocumento1 páginaPatient Type: OPD: TSH Test ReportVeenu SehrawatAinda não há avaliações
- Trigeminal NerveDocumento39 páginasTrigeminal NerveKamlesh DuggaAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Anterior Guidance: Group Function/canine Guidance. A Literature ReviewDocumento4 páginasAnterior Guidance: Group Function/canine Guidance. A Literature ReviewAayushi Vaidya100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- MCQ EXAMS ENT 3rd edition الهيئة السعوديةDocumento162 páginasMCQ EXAMS ENT 3rd edition الهيئة السعوديةmirumirmisha92% (13)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Intraoperative Complications: Mandibular Anterior: Intraosseous VesselsDocumento2 páginasIntraoperative Complications: Mandibular Anterior: Intraosseous VesselsRoenteiqAinda não há avaliações
- Sindrom GradenigoDocumento5 páginasSindrom GradenigoKelompok F8 CoasAinda não há avaliações
- Bailey & Love MCQs-EMQs in Surgery-Part - 2Documento10 páginasBailey & Love MCQs-EMQs in Surgery-Part - 2JockerAinda não há avaliações
- Cranial Nerves 2016-36782Documento51 páginasCranial Nerves 2016-36782Danu PostolacheAinda não há avaliações
- Different Types of Face ShapeDocumento10 páginasDifferent Types of Face ShapeJoyce Anne LlamesAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Activity 1.3.2: Student Resource SheetDocumento3 páginasActivity 1.3.2: Student Resource SheetmeowAinda não há avaliações
- AuditionDocumento35 páginasAuditionBam SeñeresAinda não há avaliações
- Imp 1Documento5 páginasImp 1pradeepgade1Ainda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Pathology of The ThyroidDocumento39 páginasPathology of The ThyroidPriiya AshiwiniAinda não há avaliações
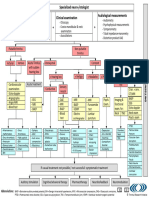
- TRI Tinnitus FlowchartDocumento1 páginaTRI Tinnitus FlowchartAdvocacia VitóriaAinda não há avaliações
- Universal Numbering Systemwide - WikipediaDocumento11 páginasUniversal Numbering Systemwide - WikipediaMuhammad SidddiqueAinda não há avaliações
- Rottweiler Breed StandardDocumento5 páginasRottweiler Breed StandardArya WiratamaAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Icd X: Diagnose ICD Diagnosa ICDDocumento33 páginasIcd X: Diagnose ICD Diagnosa ICDannisa statiraAinda não há avaliações
- Kadasne's Textbook of Anatomy (Clinically Oriented) VOLUME 3 Head, Neck, Face and Brain (2009) (PDF) (UnitedVRG)Documento365 páginasKadasne's Textbook of Anatomy (Clinically Oriented) VOLUME 3 Head, Neck, Face and Brain (2009) (PDF) (UnitedVRG)Ahmad YAinda não há avaliações