Você também pode gostar
- Shock: Rahayu Setyowati Bachelor of Nursing, Padjadjaran University IndonesiaDocumento35 páginasShock: Rahayu Setyowati Bachelor of Nursing, Padjadjaran University IndonesiazafranAinda não há avaliações
- ShockDocumento75 páginasShockaulianmediansyahAinda não há avaliações
- ShockDocumento49 páginasShockpaulyn ramos100% (1)
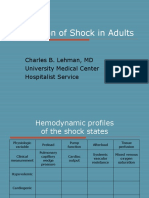
- Evaluation of Shock in AdultsDocumento99 páginasEvaluation of Shock in AdultsekramsAinda não há avaliações
- Shock: Ibrahim Ali & Winfred C. ParnellDocumento30 páginasShock: Ibrahim Ali & Winfred C. ParnellsgolbariAinda não há avaliações
- Respiratory FailureDocumento22 páginasRespiratory FailurereynoldAinda não há avaliações
- Hemorrhage - ShockDocumento55 páginasHemorrhage - Shocktusharbk08313100% (2)
- Post Operative HypotensionDocumento7 páginasPost Operative HypotensionbbyesAinda não há avaliações
- Acute Heart FailureDocumento9 páginasAcute Heart FailureChen Briones100% (1)
- Ratheesh R.LDocumento23 páginasRatheesh R.LvaishnaviAinda não há avaliações
- MS ReviewerDocumento158 páginasMS ReviewerDexan Juridico100% (2)
- Respiratory Emergency 2019Documento24 páginasRespiratory Emergency 2019bayuAinda não há avaliações
- Respiratory Failure (Aan) PDFDocumento19 páginasRespiratory Failure (Aan) PDFYudionoAinda não há avaliações
- Respiratory Failure (Aan) PDFDocumento19 páginasRespiratory Failure (Aan) PDFYudionoAinda não há avaliações
- Neonatal EmergenciesDocumento123 páginasNeonatal EmergenciesMaria Babette Almazan Talavera100% (2)
- Approach To Dyspnea: Dr. Ghulam Hussain Baloch Associate Professor of Medicine LUMHS, JamshoroDocumento48 páginasApproach To Dyspnea: Dr. Ghulam Hussain Baloch Associate Professor of Medicine LUMHS, JamshoroAndita Delifauzan SyabanaAinda não há avaliações
- Congestive Heart FailureDocumento6 páginasCongestive Heart Failureseigelystic100% (1)
- Hypotension & ShockDocumento22 páginasHypotension & ShockEkawati ErprismanAinda não há avaliações
- Schwartz: ShockDocumento55 páginasSchwartz: ShockJovy Tan-Amodia100% (9)
- Lecturer: Idol L. Bondoc, M.D.,R.NDocumento58 páginasLecturer: Idol L. Bondoc, M.D.,R.NidolbondocAinda não há avaliações
- Sinaia 2 Oct 2014 - Final-Acute Heart FailureDocumento285 páginasSinaia 2 Oct 2014 - Final-Acute Heart FailureBogdanel MihaiAinda não há avaliações
- Biologic CrisisDocumento242 páginasBiologic CrisismajAinda não há avaliações
- DYSPNEADocumento37 páginasDYSPNEAdr. snehal patilAinda não há avaliações
- Resuscitation and Shock: LSU Medical Student Clerkship, New Orleans, LADocumento40 páginasResuscitation and Shock: LSU Medical Student Clerkship, New Orleans, LAFarazAinda não há avaliações
- Nean Salubre-Ansale, RN: CU, Clinical InstructorDocumento23 páginasNean Salubre-Ansale, RN: CU, Clinical InstructorNean Salubre AnsaleAinda não há avaliações
- Shock Management, by Ayman RawehDocumento15 páginasShock Management, by Ayman RawehaymxAinda não há avaliações
- Respiratory Assessment: - AirwayDocumento40 páginasRespiratory Assessment: - AirwayTri Fitria RamadhanAinda não há avaliações
- ShockDocumento20 páginasShockعبدالواسع الاهنوميAinda não há avaliações
- Shock KGD SMT 7 PDFDocumento86 páginasShock KGD SMT 7 PDFTikuqNyukUnyukUnyukAinda não há avaliações
- Congestive Heart Failure in ChildrenDocumento48 páginasCongestive Heart Failure in ChildrenSalman KhanAinda não há avaliações
- Introduction To ShockDocumento56 páginasIntroduction To ShockPaolo VegaAinda não há avaliações
- (Pathophysiology, Types & MGT) : ShockDocumento37 páginas(Pathophysiology, Types & MGT) : ShockApriliani Nur Puspita SariAinda não há avaliações
- Pulmonary EmbolismDocumento21 páginasPulmonary EmbolismChoga Ilham ArlandoAinda não há avaliações
- Care of A Child With Cardiovascular DysfunctionDocumento71 páginasCare of A Child With Cardiovascular DysfunctionMorgan Mitchell100% (1)
- Pericarditis and Pericardial EffusionDocumento31 páginasPericarditis and Pericardial EffusionDedy Chandra HariyonoAinda não há avaliações
- I. Acute Heart Failure: What Every Physician Needs To KnowDocumento13 páginasI. Acute Heart Failure: What Every Physician Needs To KnowRubie Ann TillorAinda não há avaliações
- Shock & Iv Fluids: Dr. Ahmed Khan Sangrasi Associate Professor, Department of Surgery, LUMHS JamshoroDocumento120 páginasShock & Iv Fluids: Dr. Ahmed Khan Sangrasi Associate Professor, Department of Surgery, LUMHS JamshoroTheruna100% (1)
- Shock: By: Dr. Samer Sabri M.B.CH.B F.I.C.M.SDocumento34 páginasShock: By: Dr. Samer Sabri M.B.CH.B F.I.C.M.Ssamer falconAinda não há avaliações
- 12 Resuscitation With CPR FinalDocumento19 páginas12 Resuscitation With CPR FinalAnjela Fae Jintalan AmadorAinda não há avaliações
- Cardinal Presentations Guide Hsas 21.11.2019Documento20 páginasCardinal Presentations Guide Hsas 21.11.2019Nurhafizah IbrahimAinda não há avaliações
- Fluid, Electrolyte, Acid and Base Imbalances-1-1Documento67 páginasFluid, Electrolyte, Acid and Base Imbalances-1-1Muhammad AsifAinda não há avaliações
- Acute Trauma Care:: ShockDocumento45 páginasAcute Trauma Care:: ShockGeoffrey100% (1)
- KP 2.5.5.4 112027 - Shock FKGDocumento39 páginasKP 2.5.5.4 112027 - Shock FKGnurul ramadhiniAinda não há avaliações
- Shock Types 141009102815 Conversion Gate01Documento41 páginasShock Types 141009102815 Conversion Gate01Samjaisheel SamsonAinda não há avaliações
- Module 3 A PresentationDocumento79 páginasModule 3 A PresentationJesus William Arizapana MamaniAinda não há avaliações
- Pulmonary Embolism Postpartum PIH 2022Documento19 páginasPulmonary Embolism Postpartum PIH 2022Nikky SilvestreAinda não há avaliações
- Shock, Hypovolemic, AnaphylacticDocumento17 páginasShock, Hypovolemic, Anaphylacticmhmdalbdyny764Ainda não há avaliações
- Heart FailureDocumento47 páginasHeart Failureedry901Ainda não há avaliações
- May Worsen With Abdo Contraction Cough: Reverse AnticoagulationDocumento7 páginasMay Worsen With Abdo Contraction Cough: Reverse AnticoagulationActeen Myoseen100% (1)
- Under Supervision DR/ Mariam Sabry: Ulmonary DemaDocumento28 páginasUnder Supervision DR/ Mariam Sabry: Ulmonary DemaMohamed ElsyaedAinda não há avaliações
- Respiratory Failure Workup: Approach ConsiderationsDocumento8 páginasRespiratory Failure Workup: Approach Considerationsjeanie mae PangapalanAinda não há avaliações
- H and T of ACLSDocumento1 páginaH and T of ACLSmunkeebusinessAinda não há avaliações
- Shock Study GuideDocumento8 páginasShock Study GuideMadameb1Ainda não há avaliações
- Rheumatic Fever and Rheumatic CarditisDocumento8 páginasRheumatic Fever and Rheumatic CarditisDyanne Tan DabuAinda não há avaliações
- 16 Amniotic Fluid EmbolismDocumento46 páginas16 Amniotic Fluid EmbolismAhmed TarigAinda não há avaliações
- Acute Pulmonary Edema: Purwoko Sugeng HDocumento25 páginasAcute Pulmonary Edema: Purwoko Sugeng HBee DanielAinda não há avaliações
- Shock Pathophysiology and ManagementDocumento27 páginasShock Pathophysiology and ManagementAadal NayyarAinda não há avaliações
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtNo EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtNota: 5 de 5 estrelas5/5 (1)
- Nursing: Lab Values: a QuickStudy Laminated 6-Page Reference GuideNo EverandNursing: Lab Values: a QuickStudy Laminated 6-Page Reference GuideAinda não há avaliações
- An Authentic Ecg SimulatorDocumento118 páginasAn Authentic Ecg SimulatorbioAinda não há avaliações
- Transfusion of RBCDocumento2 páginasTransfusion of RBCwilzmaxAinda não há avaliações
- Reynaud's DiseaseDocumento13 páginasReynaud's Diseasezebzeb STEMAAinda não há avaliações
- The Use of Svo2 Monitoring in The Cardiac Intensive Care UnitDocumento60 páginasThe Use of Svo2 Monitoring in The Cardiac Intensive Care UnitAnthony RossiAinda não há avaliações
- Child Health NursingDocumento5 páginasChild Health Nursingprincipalnursing rampurhat 2023Ainda não há avaliações
- Hes 005 Session 14sasDocumento8 páginasHes 005 Session 14sasJose Melmar Autida AutenticoAinda não há avaliações
- 7-Action Drugs On BP in Intact RabbitDocumento16 páginas7-Action Drugs On BP in Intact Rabbitxq qxAinda não há avaliações
- Bachelor of Medical Lab. Technology-BmltDocumento33 páginasBachelor of Medical Lab. Technology-BmltSantosh KanelAinda não há avaliações
- 04.0 HydrocephalusDocumento41 páginas04.0 HydrocephalusBaraka SayoreAinda não há avaliações
- Digestive GlandsDocumento17 páginasDigestive GlandsPrazwal RegmiAinda não há avaliações
- Drug Study For PneumoniaDocumento15 páginasDrug Study For PneumoniaPrincess Pauline Abrasaldo100% (1)
- Pathophysiology of Acute Ischemic Heart DiseaseDocumento1 páginaPathophysiology of Acute Ischemic Heart DiseaseAbie Jean BalbontinAinda não há avaliações
- Pregnancy Hypertension: An International Journal of Women's Cardiovascular HealthDocumento8 páginasPregnancy Hypertension: An International Journal of Women's Cardiovascular HealthIsmael RoseroAinda não há avaliações
- Endothelium in Health and Diseases: Dr. Meghana .P PG in PathologyDocumento57 páginasEndothelium in Health and Diseases: Dr. Meghana .P PG in Pathologynnn nnnAinda não há avaliações
- Visual Mnemonics For Pathology: Marbas, Laurie LDocumento3 páginasVisual Mnemonics For Pathology: Marbas, Laurie LusamaAinda não há avaliações
- MnemonicsDocumento4 páginasMnemonicsKarol Delagana67% (3)
- Neurology SlidesDocumento38 páginasNeurology Slidesdrmalsharrakhi_32794Ainda não há avaliações
- Why Cholesterol Is Not The Cause of Heart DiseaseDocumento2 páginasWhy Cholesterol Is Not The Cause of Heart Diseasejacksparrow2Ainda não há avaliações
- WBI01 01 Que 20180109Documento24 páginasWBI01 01 Que 20180109Anonymous D2HJ7g4OAinda não há avaliações
- Heart DiseaseDocumento40 páginasHeart DiseaseAhmer TahirAinda não há avaliações
- ASMPH Pulmo Histo Lab ImagesDocumento58 páginasASMPH Pulmo Histo Lab ImagesKatAinda não há avaliações
- Siemens SyngoviaDocumento28 páginasSiemens Syngoviashadab0123Ainda não há avaliações
- Symptoms and Signs: Compartment SyndromeDocumento4 páginasSymptoms and Signs: Compartment SyndromeajeikoAinda não há avaliações
- Blood TranfusionDocumento18 páginasBlood TranfusionVishnu PriyaAinda não há avaliações
- Thrombocytopenia in Pregnancy.Documento22 páginasThrombocytopenia in Pregnancy.kanyAinda não há avaliações
- 1e3rd - Medication NotesDocumento35 páginas1e3rd - Medication NotesKen LaguiabAinda não há avaliações
- Medical Training: - Ventilation Options - For Internal Use OnlyDocumento43 páginasMedical Training: - Ventilation Options - For Internal Use OnlyKamel HadyAinda não há avaliações
- The Effects of SmokingDocumento2 páginasThe Effects of SmokingNino-prexy AcdalAinda não há avaliações
- UnknownDocumento477 páginasUnknownCatinca DobroghiiAinda não há avaliações
- MC I Modular Reviewer Urinary SystemDocumento12 páginasMC I Modular Reviewer Urinary SystemSteiner LimAinda não há avaliações