Você também pode gostar
- Corynebacterium and ListeriaDocumento13 páginasCorynebacterium and ListeriaNuura jeylani KasimAinda não há avaliações
- BLOOD LECTURE 4 2017 Immunity 1Documento38 páginasBLOOD LECTURE 4 2017 Immunity 1Philip Abayomi VincentAinda não há avaliações
- TransplantationpptfinalDocumento57 páginasTransplantationpptfinalmilka berhaneAinda não há avaliações
- Vaccine Chapter-4Documento64 páginasVaccine Chapter-4jihovajayraAinda não há avaliações
- C. Tetani FinalDocumento3 páginasC. Tetani FinalSajjad Hossain ShuvoAinda não há avaliações
- Course 11 - ImunochemistryDocumento31 páginasCourse 11 - ImunochemistryPopa NicuAinda não há avaliações
- Innate & Adaptive Immunity: Innate Immunity Exposure To The Microbe (Antigen) - It Is Nonspecific andDocumento14 páginasInnate & Adaptive Immunity: Innate Immunity Exposure To The Microbe (Antigen) - It Is Nonspecific andSAKARIYE MAXAMEDAinda não há avaliações
- Course ReviewDocumento17 páginasCourse Reviewانس احمدAinda não há avaliações
- Immunologic Tolerance and AutoimmunityDocumento41 páginasImmunologic Tolerance and AutoimmunityNana KembangkempisAinda não há avaliações
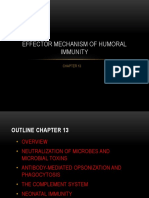
- Effector Mechanism of Humoral ImmunityDocumento40 páginasEffector Mechanism of Humoral ImmunityMiss AisyahAinda não há avaliações
- Summary of Chapter 4 Diseases of The Immune System: Innate and Adaptive ImmunityDocumento8 páginasSummary of Chapter 4 Diseases of The Immune System: Innate and Adaptive ImmunityBadda casAinda não há avaliações
- Immunity 2022Documento53 páginasImmunity 2022Craft Hachz By dhiyaAinda não há avaliações
- Pharmacology 2Documento26 páginasPharmacology 2Subham SinghAinda não há avaliações
- MedMic Midterm ReviewDocumento23 páginasMedMic Midterm ReviewQuan ThieuAinda não há avaliações
- Diseases of The Immune SystemDocumento65 páginasDiseases of The Immune Systemanon_62816775Ainda não há avaliações
- Bookshelf: Chapter 8specific Acquired ImmunityDocumento12 páginasBookshelf: Chapter 8specific Acquired ImmunityBlake KamminAinda não há avaliações
- Mechanism of Immune SystemsDocumento23 páginasMechanism of Immune SystemsRoslinda Bt Abd RazakAinda não há avaliações
- 1.4 - ClostridiumDocumento45 páginas1.4 - Clostridiumsajad abasAinda não há avaliações
- Host Defense Against Viral Infection-AnimalsDocumento38 páginasHost Defense Against Viral Infection-AnimalsalishbaAinda não há avaliações
- Basic Immunology OverviewDocumento51 páginasBasic Immunology OverviewEstee van WykAinda não há avaliações
- Host Immune Response To Periodontal PathogensDocumento42 páginasHost Immune Response To Periodontal Pathogensjamaica faith ramonAinda não há avaliações
- Lecture 1Documento52 páginasLecture 1Emmanuel Thon MadingAinda não há avaliações
- Presentation of MicrobiologyDocumento18 páginasPresentation of MicrobiologyAnant kushwahaAinda não há avaliações
- Immunity To MicrobesDocumento65 páginasImmunity To Microbesmulatumelese100% (1)
- How Microorganism Cause DiseaseDocumento16 páginasHow Microorganism Cause DiseaseMARTINEZ JUSTINEAinda não há avaliações
- Inmunidad Innata ActorDocumento50 páginasInmunidad Innata ActorBreen PhAinda não há avaliações
- Immune Responses To Human Papillomavirus: Margaret StanleyDocumento7 páginasImmune Responses To Human Papillomavirus: Margaret StanleyDina A. ŠabićAinda não há avaliações
- Edexcel (A) Biology A-level Topic 6: Immunity, Infection and Forensics NotesDocumento8 páginasEdexcel (A) Biology A-level Topic 6: Immunity, Infection and Forensics NoteshtbfdgAinda não há avaliações
- Understanding the Complement System's Role in ImmunityDocumento70 páginasUnderstanding the Complement System's Role in ImmunitySarvesh PatilAinda não há avaliações
- Vaccines1 03Documento41 páginasVaccines1 03Aasim HabibAinda não há avaliações
- Immunosuppressive AgentsDocumento62 páginasImmunosuppressive AgentsApurba Sarker ApuAinda não há avaliações
- Innate and adaptive immunity defensesDocumento63 páginasInnate and adaptive immunity defensesSarvesh Patil100% (1)
- 53Documento29 páginas53Keerthy Venthen100% (1)
- Immunopathology 2022Documento51 páginasImmunopathology 2022ahed almatarAinda não há avaliações
- Bacterial ToxinsDocumento3 páginasBacterial ToxinsMoh'd GhanayemAinda não há avaliações
- Cell Mediated and Humoral Immunity. Cytokines & The Immune Responses, Hypersensitivity ReactionsDocumento40 páginasCell Mediated and Humoral Immunity. Cytokines & The Immune Responses, Hypersensitivity ReactionsAjaga RuqayyahAinda não há avaliações
- SGD 21 - Immunology 1Documento7 páginasSGD 21 - Immunology 1John RayAinda não há avaliações
- Immunopotentiation: Immunopotentiation Can Be Defined As The ProcessDocumento67 páginasImmunopotentiation: Immunopotentiation Can Be Defined As The ProcesssamyAinda não há avaliações
- Pathology of InfectionsDocumento22 páginasPathology of InfectionsAadi VashishthaAinda não há avaliações
- Immunology & Immunopathology: Key Immune ResponsesDocumento43 páginasImmunology & Immunopathology: Key Immune Responsesdogzmania4ever7270Ainda não há avaliações
- Immune Thrombocytopenia Purpura: Clinical PathwayDocumento6 páginasImmune Thrombocytopenia Purpura: Clinical PathwayAsterlyn ConiendoAinda não há avaliações
- SGD 23 - Immunology 3Documento4 páginasSGD 23 - Immunology 3John RayAinda não há avaliações
- Immunology Flash CardsDocumento46 páginasImmunology Flash CardsRickyNoviantoAinda não há avaliações
- MHC I Proteins, Which Present Antigens To Cytotoxic T Cells, (2) MHC II Proteins, Which Present Antigens T Helper CellsDocumento25 páginasMHC I Proteins, Which Present Antigens To Cytotoxic T Cells, (2) MHC II Proteins, Which Present Antigens T Helper CellsMudassar Roomi100% (1)
- Cell Mediated Immunity: Department of Parasitology, Medical Faculty, Hasanuddin UniversityDocumento64 páginasCell Mediated Immunity: Department of Parasitology, Medical Faculty, Hasanuddin Universityintan yusufAinda não há avaliações
- The Allergic Response: Kathleen Nicole B. Bidua First Year ResidentDocumento44 páginasThe Allergic Response: Kathleen Nicole B. Bidua First Year ResidentNicole BiduaAinda não há avaliações
- Sistem LimpaDocumento65 páginasSistem LimpaXenaAinda não há avaliações
- The Immune System: Cells and Their FunctionsDocumento49 páginasThe Immune System: Cells and Their FunctionsUmer YasirAinda não há avaliações
- Immunochemistry 1Documento51 páginasImmunochemistry 1RuthAinda não há avaliações
- 10 - Defenses Against Disease - Week8 - DrNyembe - 2022Documento26 páginas10 - Defenses Against Disease - Week8 - DrNyembe - 2022Muke MpilwenhleAinda não há avaliações
- Understanding the Basics of ImmunologyDocumento64 páginasUnderstanding the Basics of ImmunologySasidhar VajralaAinda não há avaliações
- Summary Notes - Topic 6 Edexcel (A) Biology A-LevelDocumento8 páginasSummary Notes - Topic 6 Edexcel (A) Biology A-LevelmohammedAinda não há avaliações
- Clostridium TetaniDocumento15 páginasClostridium TetaniAishwarya Prabhakaran100% (1)
- 2 Immune System TEMDocumento86 páginas2 Immune System TEMJiefontane AstorAinda não há avaliações
- Basic ImmunologyDocumento12 páginasBasic Immunologyjony_phurailatpamAinda não há avaliações
- AP 305 - Lecture 9 (Chapter 5) - Innate Immune Responces (Autosaved)Documento19 páginasAP 305 - Lecture 9 (Chapter 5) - Innate Immune Responces (Autosaved)Christopher MdudaAinda não há avaliações
- INIM0011A6UC - 2021 - B1 Paper HandoutDocumento11 páginasINIM0011A6UC - 2021 - B1 Paper HandoutASDAinda não há avaliações
- ImmunosuppressantsDocumento18 páginasImmunosuppressantsomar khanAinda não há avaliações
- Transfer Factors: Properties, Mechanism of Action and Its Clinical ApplicationsNo EverandTransfer Factors: Properties, Mechanism of Action and Its Clinical ApplicationsAinda não há avaliações
- SSC (Tech) - 48-106821 12 8 2016Documento5 páginasSSC (Tech) - 48-106821 12 8 2016Pragya Prakash0% (1)
- Bacterial Toxin VaccinesDocumento24 páginasBacterial Toxin VaccinesPragya PrakashAinda não há avaliações
- Tumor ImmunologyDocumento47 páginasTumor ImmunologyPragya PrakashAinda não há avaliações
- Tumor ImmunologyDocumento47 páginasTumor ImmunologyPragya PrakashAinda não há avaliações
- Review General & USMLE Microbiology MCQsDocumento51 páginasReview General & USMLE Microbiology MCQsM7md AllahhamAinda não há avaliações
- What makes a pathogenDocumento7 páginasWhat makes a pathogenSantosh BhandariAinda não há avaliações
- Bacteria and Disease - 115911Documento12 páginasBacteria and Disease - 115911Orland HarryAinda não há avaliações
- MicrobiologyDocumento81 páginasMicrobiologyAmanuel MaruAinda não há avaliações
- Micro Bacteriology PDFDocumento4 páginasMicro Bacteriology PDFMasroor ShahAinda não há avaliações
- Corynebacterium Diphtheria: Zainab A. AldhaherDocumento41 páginasCorynebacterium Diphtheria: Zainab A. Aldhaherمروه عماد عيسىAinda não há avaliações
- Agen Infeksius & Mek. Penyakit Infeksi-Ellyta 2020Documento216 páginasAgen Infeksius & Mek. Penyakit Infeksi-Ellyta 2020Agnes Zefanya Haulia NainggolanAinda não há avaliações
- USMLE Step 1 First Aid 2020 30th - MICROBIOLOGYDocumento82 páginasUSMLE Step 1 First Aid 2020 30th - MICROBIOLOGYArt PuffAinda não há avaliações
- The Pre-Tox Protocol How To Prepare Your Body For DetoxificationDocumento13 páginasThe Pre-Tox Protocol How To Prepare Your Body For DetoxificationSabrinaHaldemannAinda não há avaliações
- 1 Aa Tesis Aravena Roman Maximiliano 2015Documento339 páginas1 Aa Tesis Aravena Roman Maximiliano 2015iqyuwidya100% (1)
- Topics List - First AID 2019Documento28 páginasTopics List - First AID 2019saraAinda não há avaliações
- Arab Board Orthopedic Exam June 2013Documento35 páginasArab Board Orthopedic Exam June 2013Nasser AlbaddaiAinda não há avaliações
- Gram-Positive Cocci and Rods: Key Features, Diseases, and TreatmentsDocumento27 páginasGram-Positive Cocci and Rods: Key Features, Diseases, and TreatmentsDjdjjd SiisusAinda não há avaliações
- Chapter 18 VaccinesDocumento29 páginasChapter 18 Vaccineshusseinabdullahahmad99Ainda não há avaliações
- Microbiology AssignmentsDocumento28 páginasMicrobiology AssignmentsDavid lufafaAinda não há avaliações
- Food Spoilage: (C) PDST Home EconomicsDocumento12 páginasFood Spoilage: (C) PDST Home EconomicsJeniefer MansatAinda não há avaliações
- Chapter Two Micro 303-محولDocumento12 páginasChapter Two Micro 303-محولshimaa dewedarAinda não há avaliações
- Infection Control and Prevention in 40 CharactersDocumento23 páginasInfection Control and Prevention in 40 CharactersDrexel Faculty Esrat IslamAinda não há avaliações
- Bacterial Cell Structure, Physiology, Metabolism, and GeneticsDocumento91 páginasBacterial Cell Structure, Physiology, Metabolism, and GeneticsLindsay OttoAinda não há avaliações
- Butchering Smoking Curimg PDFDocumento446 páginasButchering Smoking Curimg PDFWaleed Bin Mosam Khattak100% (3)
- JAT - CHT 13Documento68 páginasJAT - CHT 13j_smith24Ainda não há avaliações
- USMLE Practice Questions on BacteriologyDocumento67 páginasUSMLE Practice Questions on BacteriologyKiran KrupaAinda não há avaliações
- EDTNA/ERCA Guidelines for Microbial Contamination ControlDocumento14 páginasEDTNA/ERCA Guidelines for Microbial Contamination ControlDavid VertongenAinda não há avaliações
- Microbiology Final Exam MaterialDocumento37 páginasMicrobiology Final Exam MaterialEdgar Mandeng100% (1)
- Koch's Postulates and the Chain of InfectionDocumento7 páginasKoch's Postulates and the Chain of InfectionHERRERA, ANGELAAinda não há avaliações
- Student Notes: Micro 1: Davao Doctors College Medical Laboratory Science DepartmentDocumento5 páginasStudent Notes: Micro 1: Davao Doctors College Medical Laboratory Science DepartmentMelody Jane PardilloAinda não há avaliações
- Communicable Disease NursingDocumento44 páginasCommunicable Disease NursingFreeNursingNotes100% (17)
- Antigens: Jardine Jade Albert C. Valdez, RMT Lecturer/Clinical Instructor Capitol Medical Center CollegeDocumento24 páginasAntigens: Jardine Jade Albert C. Valdez, RMT Lecturer/Clinical Instructor Capitol Medical Center CollegeMera MendozaAinda não há avaliações
- Microbiology McqsDocumento8 páginasMicrobiology McqsRimsha Naveed100% (1)
- Systemic BacteriologyDocumento101 páginasSystemic BacteriologyKanis FatemaAinda não há avaliações