Você também pode gostar
- Treatment Modalities For Mood DisordersDocumento55 páginasTreatment Modalities For Mood DisordersGlory MimiAinda não há avaliações
- Antidepressants MaterialDocumento5 páginasAntidepressants MaterialxyzAinda não há avaliações
- AntidepressantsDocumento59 páginasAntidepressantsanon_189054600100% (2)
- PsychopharmacologyDocumento32 páginasPsychopharmacologyCms CSU100% (1)
- 4.2 Psychotropic Drugs Used in PsychiatryDocumento32 páginas4.2 Psychotropic Drugs Used in PsychiatryAmar Nur Arif ZazuliAinda não há avaliações
- Types of DepressionDocumento12 páginasTypes of DepressionKADAMBARIAinda não há avaliações
- Current Clinical Strategies: Handbook of Psychiatric DrugsDocumento72 páginasCurrent Clinical Strategies: Handbook of Psychiatric Drugsmike116Ainda não há avaliações
- PA 644 - M2 LecturesDocumento412 páginasPA 644 - M2 LectureskatAinda não há avaliações
- Psycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsDocumento29 páginasPsycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsPoonam RanaAinda não há avaliações
- Antidepressant DrugsDocumento21 páginasAntidepressant DrugsKashis SharmaAinda não há avaliações
- Anti Depressants FinalDocumento61 páginasAnti Depressants FinalAuthor Nauman Shad100% (1)
- Drug Abuse and Drug Dependence: DR Keli F Med III LecturesDocumento49 páginasDrug Abuse and Drug Dependence: DR Keli F Med III LecturestheintrovAinda não há avaliações
- Nicotine Related DisordersDocumento74 páginasNicotine Related DisordersKuldeep singhAinda não há avaliações
- Moca Vs MMSEDocumento2 páginasMoca Vs MMSEYw LiuAinda não há avaliações
- Psychopharmacology NewestDocumento43 páginasPsychopharmacology NewestRegina PunAinda não há avaliações
- Antidepressants and AntipsychoticsDocumento50 páginasAntidepressants and AntipsychoticsPintu Bhushan MitraAinda não há avaliações
- Substance Use DisordersDocumento28 páginasSubstance Use DisordersAbdul NazarAinda não há avaliações
- Neuroleptics & AnxiolyticsDocumento65 páginasNeuroleptics & AnxiolyticsAntonPurpurovAinda não há avaliações
- Etiopathogenesis of DeliriumDocumento36 páginasEtiopathogenesis of DeliriumAarti Gupta100% (1)
- DELIRIUM PresentationDocumento26 páginasDELIRIUM PresentationAnkush Sharma100% (1)
- CEP BPSD Discussion Guide ENG RFCG Updated2019 PDFDocumento8 páginasCEP BPSD Discussion Guide ENG RFCG Updated2019 PDFM.DalaniAinda não há avaliações
- "Neurotransmitter": Supporting Lecturer: NOVIA SINATA, M.Si, AptDocumento24 páginas"Neurotransmitter": Supporting Lecturer: NOVIA SINATA, M.Si, AptAmoxicilliartha RivanolaAinda não há avaliações
- Geriatric Giants - DR SeymourDocumento108 páginasGeriatric Giants - DR SeymourSharon Mallia100% (1)
- Medical Mimics 2016Documento24 páginasMedical Mimics 2016Susan Redmond-VaughtAinda não há avaliações
- Delirium: EpidemiologyDocumento8 páginasDelirium: EpidemiologyNunuAinda não há avaliações
- INTRODUCTION TO NEUROPHARMACOLOGYyyDocumento27 páginasINTRODUCTION TO NEUROPHARMACOLOGYyyEbad RazviAinda não há avaliações
- Cognitive Disorders PresentationDocumento70 páginasCognitive Disorders PresentationWasiu AfoloabiAinda não há avaliações
- Sudden Onset (Within 2 Weeks) of at Least One of TheDocumento2 páginasSudden Onset (Within 2 Weeks) of at Least One of TheNeicole BandalaAinda não há avaliações
- Summary of Product Characteristics: PosologyDocumento9 páginasSummary of Product Characteristics: Posologyddandan_2Ainda não há avaliações
- Tranylcypromine in Mind Part II - Review of Clinical PH - 2017 - European Neuro PDFDocumento18 páginasTranylcypromine in Mind Part II - Review of Clinical PH - 2017 - European Neuro PDFdanilomarandolaAinda não há avaliações
- Pharmacology Workbook Class of 20 20: (Revised: March, 2018)Documento22 páginasPharmacology Workbook Class of 20 20: (Revised: March, 2018)Navdeep RandhawaAinda não há avaliações
- Assessment and Management of Agitation in Psychiatry Expert ConsensusDocumento44 páginasAssessment and Management of Agitation in Psychiatry Expert ConsensusPablo RamirezAinda não há avaliações
- Receptors Ionchannel TransporterDocumento58 páginasReceptors Ionchannel TransporterDeepu Vijay100% (1)
- NeurotransmittersDocumento29 páginasNeurotransmittersashupathakaAinda não há avaliações
- Neurobiology and BehaviorDocumento24 páginasNeurobiology and BehaviorNaveen Eldose100% (1)
- TramadolDocumento3 páginasTramadolKaren Viviene Aberilla CincoAinda não há avaliações
- AnxietyDocumento5 páginasAnxietyJohn HolmesAinda não há avaliações
- Chapter 7 Study GuideDocumento4 páginasChapter 7 Study GuidejbradeeAinda não há avaliações
- Mental Health - PsychopharmacologyDocumento4 páginasMental Health - PsychopharmacologyRenetria DrakeAinda não há avaliações
- Anti PsychoticsDocumento34 páginasAnti Psychotics88AKKAinda não há avaliações
- Investigations in PsychiatryDocumento59 páginasInvestigations in Psychiatrykiran mahal100% (1)
- Anidepressant Drugs: Pratik KhanalDocumento37 páginasAnidepressant Drugs: Pratik KhanalPratik Khanal100% (1)
- Antidepressant AgentsDocumento38 páginasAntidepressant AgentsdidiAinda não há avaliações
- Tranylcypromine in Mind Part I - Review of P - 2017 - European Neuropsychopharm PDFDocumento17 páginasTranylcypromine in Mind Part I - Review of P - 2017 - European Neuropsychopharm PDFdanilomarandolaAinda não há avaliações
- Sample Pages of Pharmacology 4th EditionDocumento25 páginasSample Pages of Pharmacology 4th EditionskAinda não há avaliações
- Neurotransmitters in Schizophrenia: Dr. Adel El SheshaiDocumento47 páginasNeurotransmitters in Schizophrenia: Dr. Adel El SheshaielvinegunawanAinda não há avaliações
- Anti-Depressants: Soumya Mary 1 Year MSC (N)Documento22 páginasAnti-Depressants: Soumya Mary 1 Year MSC (N)Salman HabeebAinda não há avaliações
- Inhibitors of MAO-A and MAO-B in Psychiatry and NeurologyDocumento27 páginasInhibitors of MAO-A and MAO-B in Psychiatry and NeurologySergeyAinda não há avaliações
- Glutamate & Gaba: NeurotransmittersDocumento33 páginasGlutamate & Gaba: NeurotransmittersPanchitaJuarezAinda não há avaliações
- Drugs For NeurolepticsDocumento1 páginaDrugs For Neurolepticssyamil_daudAinda não há avaliações
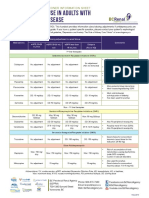
- Antidepressant Use in Adults With Chronic Kidney DiseaseDocumento1 páginaAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- 1 - Signs and Symptoms of Mental Illness-PartDocumento49 páginas1 - Signs and Symptoms of Mental Illness-PartAljoker FarragAinda não há avaliações
- Antipsychotic or Neuroleptic DrugsDocumento12 páginasAntipsychotic or Neuroleptic Drugscamile buhanginAinda não há avaliações
- Schizophrenia: By: Zoya MoraniDocumento31 páginasSchizophrenia: By: Zoya Moranimed studentAinda não há avaliações
- PsychopharmacologyDocumento53 páginasPsychopharmacologypujarze4100% (1)
- Pristiq (Desvenlafaxine) Product Monograph For CanadaDocumento48 páginasPristiq (Desvenlafaxine) Product Monograph For CanadajennabushAinda não há avaliações
- Schizophrenia OverviewDocumento8 páginasSchizophrenia OverviewRiscky LauwAinda não há avaliações
- Drug Presentation: Manisha M.Sc. Nursing 1 Year Con IlbsDocumento57 páginasDrug Presentation: Manisha M.Sc. Nursing 1 Year Con IlbsManisha ShakyaAinda não há avaliações
- Treatment Resistant OCD .Documento55 páginasTreatment Resistant OCD .Dr viren SolankiAinda não há avaliações
- Internal Medicine - DermatologyDocumento125 páginasInternal Medicine - DermatologySoleil DaddouAinda não há avaliações
- Fluids and ElectrolytesDocumento78 páginasFluids and ElectrolytesSoleil DaddouAinda não há avaliações
- LMCC II GuideDocumento79 páginasLMCC II GuideSoleil DaddouAinda não há avaliações
- Clinical Immunology and AllergyDocumento156 páginasClinical Immunology and AllergySoleil DaddouAinda não há avaliações
- Dr. Noto ID HandoutDocumento35 páginasDr. Noto ID HandoutSoleil DaddouAinda não há avaliações
- Dr. Noto ID HandoutDocumento35 páginasDr. Noto ID HandoutSoleil DaddouAinda não há avaliações
- Excoriation (Skin-Picking) Disorder: A Systematic Review of Treatment OptionsDocumento6 páginasExcoriation (Skin-Picking) Disorder: A Systematic Review of Treatment OptionsBecados PsiquiatriaAinda não há avaliações
- Yehuda Rachel. Treating Trauma - Survivors With PTSDDocumento216 páginasYehuda Rachel. Treating Trauma - Survivors With PTSDa1esh100% (2)
- Poster-Proceedings 2016Documento441 páginasPoster-Proceedings 2016Ana Rosa González BarrosoAinda não há avaliações
- A Clinician's Guide To Systemic Sex TherapyDocumento19 páginasA Clinician's Guide To Systemic Sex TherapyTedy Crestin100% (1)
- Imitrex: (Sumatriptan) Nasal SprayDocumento25 páginasImitrex: (Sumatriptan) Nasal Spray58TRONGAinda não há avaliações
- 1103CP FavazzaDocumento6 páginas1103CP FavazzaMaría Alejandra Oyanadel GuerreroAinda não há avaliações
- Multi Functional Drugs - A Novel Concept For Psycho PharmacologyDocumento3 páginasMulti Functional Drugs - A Novel Concept For Psycho Pharmacologyrocsa11Ainda não há avaliações
- Neurobiological Bases For The Relation Betweeen Sleep and DepressionDocumento11 páginasNeurobiological Bases For The Relation Betweeen Sleep and DepressionKira ChanAinda não há avaliações
- Anti Depressants 140205003201 Phpapp01Documento27 páginasAnti Depressants 140205003201 Phpapp01Josh Schultz100% (1)
- Approach Considerations: Nita V Bhatt, MD, MPH Clinical Instructor, Resident Physician, Department ofDocumento7 páginasApproach Considerations: Nita V Bhatt, MD, MPH Clinical Instructor, Resident Physician, Department ofHiLmy ZakiyahAinda não há avaliações
- Mohandas Et Al-2013-British Journal of Dermatology PDFDocumento7 páginasMohandas Et Al-2013-British Journal of Dermatology PDFEdu SajquimAinda não há avaliações
- Medications For StutteringDocumento18 páginasMedications For StutteringSalvatore SinatraAinda não há avaliações
- More Than Human - Promise and Perils - Allen BuchananDocumento208 páginasMore Than Human - Promise and Perils - Allen BuchananPragna100% (1)
- Obsessive Compulsive Disorder Ocd 1Documento16 páginasObsessive Compulsive Disorder Ocd 1Peter SmithAinda não há avaliações
- Ajor Epressive Isorder: Marshall Cates, Angela Passero, and Jacqueline FeldmanDocumento16 páginasAjor Epressive Isorder: Marshall Cates, Angela Passero, and Jacqueline FeldmanbencleeseAinda não há avaliações
- Malandain Leo Pharmacotherapy of Sexual AddictionDocumento8 páginasMalandain Leo Pharmacotherapy of Sexual AddictionSergio De PanfilisAinda não há avaliações
- Psychopharmacology For Mental Health Professionals An Integrative Approach 2nd Edition Ebook PDFDocumento62 páginasPsychopharmacology For Mental Health Professionals An Integrative Approach 2nd Edition Ebook PDFpatrick.mcfadden11198% (42)
- Treating Panic Disorder: A Quick Reference GuideDocumento23 páginasTreating Panic Disorder: A Quick Reference GuideAntónio MartinsAinda não há avaliações
- Pathophysiology of DepressionDocumento44 páginasPathophysiology of DepressionArmando Marín FloresAinda não há avaliações
- Jetlax's CNS Pharmacology Cheat Sheet For The Philippines v6.0 at Bit - Ly - CNSPcol - See Bit - Ly - CNSHandouts For 5.0 CorrectionsDocumento61 páginasJetlax's CNS Pharmacology Cheat Sheet For The Philippines v6.0 at Bit - Ly - CNSPcol - See Bit - Ly - CNSHandouts For 5.0 CorrectionsShalimar BasmanAinda não há avaliações
- A Three-Step Synthesis of FluoxetineDocumento2 páginasA Three-Step Synthesis of FluoxetineKevin VlogsAinda não há avaliações
- p896 HhujujuDocumento8 páginasp896 HhujujuwatiAinda não há avaliações
- Dapoxetine Dosing InformationDocumento25 páginasDapoxetine Dosing InformationA.R.AthreyaAinda não há avaliações
- Adjustment Disorders and PTSDDocumento21 páginasAdjustment Disorders and PTSDAprilihardini Laksmi100% (1)
- Suicide Prevention Strategies Revisited 10-Year SystematicDocumento14 páginasSuicide Prevention Strategies Revisited 10-Year Systematicmary morelliAinda não há avaliações
- PsychopathologyDocumento14 páginasPsychopathologyKrinjal KapoorAinda não há avaliações
- Knime Analytics Platform For Data ScientistsDocumento163 páginasKnime Analytics Platform For Data Scientistsmr joneyAinda não há avaliações
- DR Walsh Autism Ocd Pandas Depression MethylationDocumento6 páginasDR Walsh Autism Ocd Pandas Depression MethylationAnupama PouloseAinda não há avaliações
- The Side Effects of Common Psychiatric DrugsDocumento40 páginasThe Side Effects of Common Psychiatric DrugsPhilip Jonkers100% (1)
- Pharma - Updated Topical Past Papers 2007-23Documento53 páginasPharma - Updated Topical Past Papers 2007-23Tayyab AfzalAinda não há avaliações