Você também pode gostar
- Carcinoma of The CervixDocumento31 páginasCarcinoma of The CervixmlinaballerinaAinda não há avaliações
- Diabetes Mellitus Nair PDFDocumento5 páginasDiabetes Mellitus Nair PDFWeng RamojalAinda não há avaliações
- 2017 EACTS Guidelines On Perioperative Medication in Adult Cardiac SurgeryDocumento29 páginas2017 EACTS Guidelines On Perioperative Medication in Adult Cardiac SurgeryGaetano Di GiovanniAinda não há avaliações
- Female GenitaliaDocumento5 páginasFemale GenitaliamlinaballerinaAinda não há avaliações
- Lung Cancer Staging Poster UpdatedDocumento2 páginasLung Cancer Staging Poster UpdatedCarlos Eduardo Avila100% (1)
- LP 4-ImmunoprophylaxisDocumento15 páginasLP 4-ImmunoprophylaxismlinaballerinaAinda não há avaliações
- Intrapartum Care: Prof. Dr. Crăiu Doru Ioan ȚDocumento65 páginasIntrapartum Care: Prof. Dr. Crăiu Doru Ioan Țmlinaballerina100% (1)
- Reproductive Physiology and AnatomyDocumento18 páginasReproductive Physiology and AnatomymlinaballerinaAinda não há avaliações
- Antenatal CareDocumento47 páginasAntenatal CaremlinaballerinaAinda não há avaliações
- Arensman - Pediatric SurgeryDocumento486 páginasArensman - Pediatric Surgeryedrons0% (1)
- Ss / Essbe Eset Mac CybersecurityDocumento1 páginaSs / Essbe Eset Mac CybersecuritymlinaballerinaAinda não há avaliações
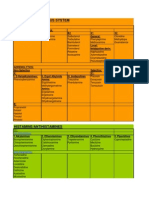
- Adrenergic Nervous System: A: Direct ActingDocumento13 páginasAdrenergic Nervous System: A: Direct ActingmlinaballerinaAinda não há avaliações
- Oxygen CascadeDocumento12 páginasOxygen Cascadehy3pjb1984Ainda não há avaliações
- Treatment Evaluation in Congenital Abdominal Wall DefectsDocumento23 páginasTreatment Evaluation in Congenital Abdominal Wall DefectsmlinaballerinaAinda não há avaliações
- Cranial Nerves-Anatomy and Clinical Comments Wilson-PauwelsDocumento189 páginasCranial Nerves-Anatomy and Clinical Comments Wilson-PauwelsAlina Elena Tudorache100% (6)
- GOUTDocumento16 páginasGOUTGabby RachediaAinda não há avaliações
- Cardiogenic ShockDocumento22 páginasCardiogenic ShockmlinaballerinaAinda não há avaliações
- FACE - FACIES Neck- thyroid examDocumento59 páginasFACE - FACIES Neck- thyroid exammlinaballerinaAinda não há avaliações
- Arterial DiseaseDocumento7 páginasArterial DiseasemlinaballerinaAinda não há avaliações
- Plasma ProteinsDocumento7 páginasPlasma ProteinsmlinaballerinaAinda não há avaliações
- RansonDocumento1 páginaRansonmlinaballerinaAinda não há avaliações
- Table 20Documento2 páginasTable 20mlinaballerinaAinda não há avaliações
- Anomalii Congenitale MinoreDocumento2 páginasAnomalii Congenitale MinoremlinaballerinaAinda não há avaliações
- Holes Cha 20 Urinary PT 2Documento6 páginasHoles Cha 20 Urinary PT 2mlinaballerinaAinda não há avaliações
- 26-02 PptlectDocumento23 páginas26-02 PptlectmlinaballerinaAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Animal Tissues Lab SlidesDocumento21 páginasAnimal Tissues Lab SlidesMichaelAinda não há avaliações
- SalmonellaDocumento14 páginasSalmonelladrparachuruAinda não há avaliações
- No Nama Barang Stok Awal Barang Masuk Barang Keluar Sisa Stock Harga SatuanDocumento16 páginasNo Nama Barang Stok Awal Barang Masuk Barang Keluar Sisa Stock Harga SatuanNurmalasari SaryAinda não há avaliações
- Chapter 1-5 PDFDocumento77 páginasChapter 1-5 PDFEstebanAinda não há avaliações
- Pregnancy Nursing Diagnosis and Care PlanDocumento12 páginasPregnancy Nursing Diagnosis and Care PlanJeane Louise PalmeroAinda não há avaliações
- AlkaloidsDocumento21 páginasAlkaloidssanjiv_m20100% (1)
- First Aid Plan ConstructionDocumento13 páginasFirst Aid Plan ConstructionUmair KhanAinda não há avaliações
- ENT Scholar Volume 1Documento93 páginasENT Scholar Volume 1Dr. T. BalasubramanianAinda não há avaliações
- Biological Psychiatry: Is There Any Other KindDocumento9 páginasBiological Psychiatry: Is There Any Other KindLiam Jacque LapuzAinda não há avaliações
- Reading and Writing: Quarter 3: Module 2 - Lesson 1Documento13 páginasReading and Writing: Quarter 3: Module 2 - Lesson 1MELANIE IBARDALOZA100% (2)
- 4 Agroecology IPMDocumento16 páginas4 Agroecology IPMZahara AmalinaAinda não há avaliações
- Snow White - Abnormal Psychology PaperDocumento6 páginasSnow White - Abnormal Psychology PaperNicky JosephAinda não há avaliações
- Vox Media KitDocumento19 páginasVox Media Kitapi-272196122Ainda não há avaliações
- ASDAS CalculatorDocumento4 páginasASDAS CalculatorSthepany HuertasAinda não há avaliações
- Body Fluids and CirculationDocumento10 páginasBody Fluids and CirculationFree4TechAinda não há avaliações
- Vermikompos and Gliocladium Effectiveness Against Fusarium WiltDocumento8 páginasVermikompos and Gliocladium Effectiveness Against Fusarium WiltJioWongMenengAinda não há avaliações
- Single Vs Multiple Visits in PulpectomyDocumento7 páginasSingle Vs Multiple Visits in PulpectomyHudh HudAinda não há avaliações
- The History, Theory and Practice of Restricted Blood Flow Resistance Training (Rbfrt/Kaatsu)Documento10 páginasThe History, Theory and Practice of Restricted Blood Flow Resistance Training (Rbfrt/Kaatsu)Fabiano LacerdaAinda não há avaliações
- CVS Drug TablesDocumento12 páginasCVS Drug TablesSaajid AmraAinda não há avaliações
- Human Longevity Project Vitality Experience Guidebook 2Documento42 páginasHuman Longevity Project Vitality Experience Guidebook 2Britt LangAinda não há avaliações
- Acupuntura - Pulso Tornozelo - InglêsDocumento40 páginasAcupuntura - Pulso Tornozelo - InglêsAntonio de AlexandreAinda não há avaliações
- ICSE X Biology Board Paper 2017 SolutionDocumento8 páginasICSE X Biology Board Paper 2017 SolutionKing YashasAinda não há avaliações
- Script For Head To NeckDocumento7 páginasScript For Head To NeckSydney Joy Abaca100% (1)
- 10 11648 J Ijde 20200502 12Documento4 páginas10 11648 J Ijde 20200502 12AdemoluAinda não há avaliações
- Pathophysiology of Ectopic PregnancyDocumento11 páginasPathophysiology of Ectopic PregnancyJann ericka JaoAinda não há avaliações
- Fibroid in WomenDocumento13 páginasFibroid in Womentnemwill1880% (5)
- Soil-less Culture Techniques for Modern AgricultureDocumento6 páginasSoil-less Culture Techniques for Modern AgricultureT. Aswini PatroAinda não há avaliações
- The Witch Trials of Finnmark, Northern NorwayDocumento14 páginasThe Witch Trials of Finnmark, Northern NorwaythestylerhimselfAinda não há avaliações
- Rice Bran Oil - Natures Gift To MankindDocumento2 páginasRice Bran Oil - Natures Gift To Mankindlehmanwolf100% (1)
- Medical Image Computing (Cap 5937)Documento44 páginasMedical Image Computing (Cap 5937)Android ApplicationsAinda não há avaliações