Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Chapter 18 Personality DisordersDocumento10 páginasChapter 18 Personality DisordersCatia Fernandes100% (2)
- Autorizacion CirugiaDocumento1 páginaAutorizacion Cirugiaanon_375322244Ainda não há avaliações
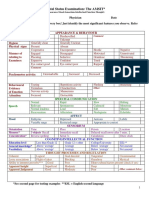
- Mental Status Examination: The AMSIT : Neat and Tidy DisshevelledDocumento2 páginasMental Status Examination: The AMSIT : Neat and Tidy Disshevellednisreen100% (1)
- Handout Knight in Rusty ArmourDocumento9 páginasHandout Knight in Rusty ArmourGobetiAinda não há avaliações
- Operations Management 6th Edition Reid Solutions ManualDocumento3 páginasOperations Management 6th Edition Reid Solutions Manuala288884902Ainda não há avaliações
- Acute Lung Injury and Ards: Andreas Crede Emergency Medicine RegistrarDocumento47 páginasAcute Lung Injury and Ards: Andreas Crede Emergency Medicine RegistrarAsri PrameswariAinda não há avaliações
- Kuliah Rematologi 5Documento17 páginasKuliah Rematologi 5Asri PrameswariAinda não há avaliações
- Kuliah Bidan - Syok HipovolemikDocumento28 páginasKuliah Bidan - Syok HipovolemikAsri PrameswariAinda não há avaliações
- Acute Respiratory Distress SyndromeDocumento77 páginasAcute Respiratory Distress SyndromeAsri PrameswariAinda não há avaliações
- Kuliah Low Back Back PainDocumento14 páginasKuliah Low Back Back PainAsri PrameswariAinda não há avaliações
- International LibraryDocumento6 páginasInternational LibraryAnonymous UbrkhAXQxAinda não há avaliações
- The Adrenal Gland: Anatomy and Hormone ProductionDocumento28 páginasThe Adrenal Gland: Anatomy and Hormone ProductionMona NasrAinda não há avaliações
- Acute Lung Injury and Ards: Andreas Crede Emergency Medicine RegistrarDocumento47 páginasAcute Lung Injury and Ards: Andreas Crede Emergency Medicine RegistrarAsri PrameswariAinda não há avaliações
- InfluenzaDocumento13 páginasInfluenzaAnonymous hkWIKjoXFVAinda não há avaliações
- Kuliah Low Back Back PainDocumento14 páginasKuliah Low Back Back PainAsri PrameswariAinda não há avaliações
- Kuliah Low Back Back PainDocumento14 páginasKuliah Low Back Back PainAsri PrameswariAinda não há avaliações
- SECTIOCAESARIANDocumento4 páginasSECTIOCAESARIANPrina Febri Atmilia100% (2)
- 4 OaDocumento37 páginas4 OaSaya MenangAinda não há avaliações
- Rheumatoid ArtritisDocumento56 páginasRheumatoid ArtritisListya NormalitaAinda não há avaliações
- Kuliah Rematologi 1Documento4 páginasKuliah Rematologi 1Asri PrameswariAinda não há avaliações
- Stages of Gross Motor Development from Infancy to Age 12Documento17 páginasStages of Gross Motor Development from Infancy to Age 12Gul RockzzAinda não há avaliações
- Introduction To AnesthesiologyDocumento68 páginasIntroduction To AnesthesiologyOzza AlhudaAinda não há avaliações
- Adult Grip Strength Norms For The Baseline Digital DynamometerDocumento25 páginasAdult Grip Strength Norms For The Baseline Digital DynamometerOmar Escalante DíazAinda não há avaliações
- Asthma Broncial (Theophylline)Documento41 páginasAsthma Broncial (Theophylline)Nadya Zahra Henni100% (1)
- Nurse ResumeDocumento1 páginaNurse Resumeapi-400113721Ainda não há avaliações
- Bolton Analysis Determines Tooth Size DiscrepanciesDocumento24 páginasBolton Analysis Determines Tooth Size DiscrepanciesmebibegAinda não há avaliações
- Geriatri 1Documento6 páginasGeriatri 1KemasNugrohoAinda não há avaliações
- Journal Prosto PDFDocumento6 páginasJournal Prosto PDFdifaAinda não há avaliações
- Nelson FNCPDocumento2 páginasNelson FNCPDenisse Shazz Mae MaretAinda não há avaliações
- CLOZE TEST Discovery Could Ease Blood ShortageDocumento2 páginasCLOZE TEST Discovery Could Ease Blood ShortageKarsan Ayaz MaierAinda não há avaliações
- How To Apply To CPA's Clinical Specialty ProgramDocumento20 páginasHow To Apply To CPA's Clinical Specialty ProgramDr Hafiz Sheraz ArshadAinda não há avaliações
- ParkinsonDocumento54 páginasParkinsonAngel YapAinda não há avaliações
- Medicare Ensures Healthcare InsuranceDocumento30 páginasMedicare Ensures Healthcare InsuranceEsquiAinda não há avaliações
- 2-McGroarty - SEMIC Rome 2016 FMGDocumento62 páginas2-McGroarty - SEMIC Rome 2016 FMGvittoria1Ainda não há avaliações
- Siemens Has Your AnswersDocumento10 páginasSiemens Has Your AnswersEduardo Saul MendozaAinda não há avaliações
- SOAP Handout 2010Documento4 páginasSOAP Handout 2010wawanAinda não há avaliações
- Jurnal Insect Bite PDFDocumento4 páginasJurnal Insect Bite PDFjihadahAinda não há avaliações
- Maintain AirwaysDocumento3 páginasMaintain AirwaysJei JayAinda não há avaliações
- Janie Jacobs Resume March 2019Documento2 páginasJanie Jacobs Resume March 2019api-404179099Ainda não há avaliações
- Professionalism in NursingDocumento7 páginasProfessionalism in NursingAngelLeeAinda não há avaliações
- Dengue Disease Spectrum Among Infants in The 2001 Dengue Epidemic in Chennai, Tamil Nadu, IndiaDocumento3 páginasDengue Disease Spectrum Among Infants in The 2001 Dengue Epidemic in Chennai, Tamil Nadu, IndiaReju VijayandranAinda não há avaliações
- Effects of Maitland Mobilization and Mul PDFDocumento6 páginasEffects of Maitland Mobilization and Mul PDFKuroha Hagane KunAinda não há avaliações
- Daptomycin (Cubicin)Documento1 páginaDaptomycin (Cubicin)Adrianne BazoAinda não há avaliações
- Cerebral ContusionDocumento88 páginasCerebral ContusionHeaAinda não há avaliações
- Infectious Diseases Consultation ReportDocumento5 páginasInfectious Diseases Consultation ReportRohitKumar100% (1)