Você também pode gostar
- K-11 Esophagus: Departemen Bedah Fakultas Kedokteran USUDocumento38 páginasK-11 Esophagus: Departemen Bedah Fakultas Kedokteran USUChristian Lumban GaolAinda não há avaliações
- Gastroesophageal Reflux DiseaseDocumento37 páginasGastroesophageal Reflux DiseaseMahad Maxamed AxmedAinda não há avaliações
- Nur 322 Gi DisordersDocumento113 páginasNur 322 Gi DisordersLovelights ZamoraAinda não há avaliações
- Kuliah Upper Gi Tract DiseaseDocumento78 páginasKuliah Upper Gi Tract DiseaseAnggun Pulihana WAinda não há avaliações
- Esophageal DisorderDocumento25 páginasEsophageal DisorderJuma AwarAinda não há avaliações
- Esophageal DisordersDocumento37 páginasEsophageal DisordersDanielle FosterAinda não há avaliações
- Powerpoint: Disorders of The EsophagusDocumento65 páginasPowerpoint: Disorders of The Esophagusj.doe.hex_8782% (11)
- Esophageal Disorder Part IIDocumento27 páginasEsophageal Disorder Part IIJuma AwarAinda não há avaliações
- GI Tract: Esophagus & StomachDocumento126 páginasGI Tract: Esophagus & StomachPablo SisirucaAinda não há avaliações
- Wa0001Documento41 páginasWa0001Riya ShindeAinda não há avaliações
- Disease of Esophagus and Hiatal HerniaDocumento76 páginasDisease of Esophagus and Hiatal HerniaSiriporn PongpattarapakAinda não há avaliações
- Dysphagia: Dr. Sangeeta Aggarwal Assistant Professor, E.N.T Deptt GMCH, PatialaDocumento29 páginasDysphagia: Dr. Sangeeta Aggarwal Assistant Professor, E.N.T Deptt GMCH, PatialaVishalAinda não há avaliações
- Surgical Diseases of The EsophagusDocumento35 páginasSurgical Diseases of The Esophagusmogesie1995Ainda não há avaliações
- Gastro-Oesophageal Reflux Disease (GORD) : Anish DhakalDocumento31 páginasGastro-Oesophageal Reflux Disease (GORD) : Anish DhakalnrauliaprtwAinda não há avaliações
- GastroenterologyDocumento94 páginasGastroenterologyAdina RomanAinda não há avaliações
- Examination of Intestinal Obstruction, Acute Abdomen and Acute Appendicitis - Eugh & BwembyaDocumento29 páginasExamination of Intestinal Obstruction, Acute Abdomen and Acute Appendicitis - Eugh & BwembyaForeighn97Ainda não há avaliações
- Small Intestine: Earle J. Niervo Medical ClerkDocumento168 páginasSmall Intestine: Earle J. Niervo Medical ClerkEarle Jimenez Niervo RNAinda não há avaliações
- Screenshot 2023-11-26 at 5.15.31 PMDocumento39 páginasScreenshot 2023-11-26 at 5.15.31 PMgauravsingh708284Ainda não há avaliações
- Lect 3 Disorder of Mouth and EsophagusDocumento42 páginasLect 3 Disorder of Mouth and EsophagusShayan ShayanAinda não há avaliações
- The Esophagus: Vic Vernenkar, D.O Department of Surgery St. Barnabas HospitalDocumento85 páginasThe Esophagus: Vic Vernenkar, D.O Department of Surgery St. Barnabas HospitalSameem MunirAinda não há avaliações
- Disorders of EsophagusDocumento19 páginasDisorders of EsophagusAjibola OlamideAinda não há avaliações
- Hiatal Hernia AchalasiaDocumento22 páginasHiatal Hernia AchalasiaDhen MarcAinda não há avaliações
- GI ReviewDocumento44 páginasGI Reviews129682Ainda não há avaliações
- Colon 2Documento56 páginasColon 2EnydLaRejAinda não há avaliações
- Esophageal Conditions: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonDocumento54 páginasEsophageal Conditions: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonVincent SerAinda não há avaliações
- Pathologies of GitDocumento50 páginasPathologies of GitSajjad AliAinda não há avaliações
- GerdDocumento37 páginasGerdAyesha ShafiqAinda não há avaliações
- Gastroesophageal Reflux Disease Gerd 1Documento62 páginasGastroesophageal Reflux Disease Gerd 1Kimverly Paredes GallanoAinda não há avaliações
- Sharpy's Surgical Series PresentationDocumento244 páginasSharpy's Surgical Series PresentationhappyhappylandAinda não há avaliações
- Icd Case No. 2Documento38 páginasIcd Case No. 2Hearty Yao100% (1)
- Group 18 Problem 1B: Thedi Darma Wijaya 405090120Documento46 páginasGroup 18 Problem 1B: Thedi Darma Wijaya 405090120mty_aldAinda não há avaliações
- Medical Surgical Nursing Module 1 Lesson 1 Upper Gastrointestinal DisordersDocumento34 páginasMedical Surgical Nursing Module 1 Lesson 1 Upper Gastrointestinal DisordersRomelyn Ordillas100% (2)
- Gastro-Esophageal Reflux Disease ( GERD)Documento31 páginasGastro-Esophageal Reflux Disease ( GERD)Malueth AnguiAinda não há avaliações
- 1100 Ultrasound of The Acute Abdomen 15 3Documento84 páginas1100 Ultrasound of The Acute Abdomen 15 3gp1promo2016Ainda não há avaliações
- Presentation On Gastric Ulcer-1Documento37 páginasPresentation On Gastric Ulcer-1Roshan GhimireAinda não há avaliações
- Peptic Ulcer: Gastritis Gastroesophageal Reflux DiseaseDocumento11 páginasPeptic Ulcer: Gastritis Gastroesophageal Reflux Diseasenickrulz10Ainda não há avaliações
- Clinical Approach To Abdominal Disorder: Kurniyanto Department of Internal MedicineDocumento68 páginasClinical Approach To Abdominal Disorder: Kurniyanto Department of Internal MedicineMonica AnggiAinda não há avaliações
- GIT DisordersDocumento171 páginasGIT DisordersKatrina PonceAinda não há avaliações
- Class 7 (G1) - GI TractDocumento112 páginasClass 7 (G1) - GI TractAdel mohammadAinda não há avaliações
- GI SlidesDDM1Documento39 páginasGI SlidesDDM1Anonymous d3qpXcm4xVAinda não há avaliações
- DYSPHAGIADocumento35 páginasDYSPHAGIAChristopher Yeoh100% (2)
- Intestinal Diseases: Gastrointestinal shengjing Hospital of Medical youwei kou (寇有为)Documento80 páginasIntestinal Diseases: Gastrointestinal shengjing Hospital of Medical youwei kou (寇有为)Abhirami AnilAinda não há avaliações
- DysphagiaDocumento35 páginasDysphagiaBashar KhalilAinda não há avaliações
- Dyspepsia FinalDocumento52 páginasDyspepsia FinalAfifah SelamatAinda não há avaliações
- Intestinal Obstruction: by Dr. Shereen Abd El-MoniemDocumento44 páginasIntestinal Obstruction: by Dr. Shereen Abd El-MoniemフセインAinda não há avaliações
- DysphagiaDocumento40 páginasDysphagiamanabdebuAinda não há avaliações
- Peptic Ulcers: DR Yotham Phiri Mmed (Surg)Documento46 páginasPeptic Ulcers: DR Yotham Phiri Mmed (Surg)Emmanuel MukukaAinda não há avaliações
- Problem 4 GIT Josephine AngeliaDocumento35 páginasProblem 4 GIT Josephine AngeliaAndreas AdiwinataAinda não há avaliações
- StomachDocumento204 páginasStomachrajmv7Ainda não há avaliações
- Surgical Disease of The Esophagus: Mahteme Bekele, MD Assistant Professor of SurgeryDocumento72 páginasSurgical Disease of The Esophagus: Mahteme Bekele, MD Assistant Professor of SurgeryBiniamAinda não há avaliações
- Oesophagus StomachDocumento28 páginasOesophagus Stomachwanja91Ainda não há avaliações
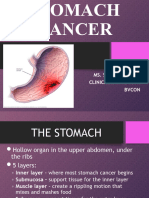
- Stomach CancerDocumento36 páginasStomach CancerSonali DakhoreAinda não há avaliações
- Peptic UlcerDocumento34 páginasPeptic UlcerAnjum AbbasiAinda não há avaliações
- Acute Abdomen: The "Black Hole" of MedicineDocumento97 páginasAcute Abdomen: The "Black Hole" of Medicineedward iskandarAinda não há avaliações
- Instestinal Obstruction UbthDocumento34 páginasInstestinal Obstruction UbthDonald IDEDEAinda não há avaliações
- Disorders of Stomach and IntestineDocumento64 páginasDisorders of Stomach and IntestineAyomide IgeAinda não há avaliações
- 4.gall StoneDocumento35 páginas4.gall Stonejitendra magarAinda não há avaliações
- Gastroesophageal RefluxDocumento20 páginasGastroesophageal Refluxtofan widyaAinda não há avaliações
- Acute Cholecystitis: Mentor: Dr. Amran Sinaga, SP.BDocumento18 páginasAcute Cholecystitis: Mentor: Dr. Amran Sinaga, SP.Bevita oktaviaAinda não há avaliações
- Pleno Pakar Drug AbuseDocumento52 páginasPleno Pakar Drug AbuseenriAinda não há avaliações
- K12 FrequencyDocumento23 páginasK12 Frequencyenri100% (1)
- (K8) Abnormality PDFDocumento22 páginas(K8) Abnormality PDFwidyamsAinda não há avaliações
- K10 Diagnosis PDFDocumento23 páginasK10 Diagnosis PDFenriAinda não há avaliações
- k11 - ScreeningDocumento12 páginask11 - ScreeningThamarai SomuAinda não há avaliações
- K10 Diagnosis PDFDocumento23 páginasK10 Diagnosis PDFenriAinda não há avaliações
- K6 RiskDocumento26 páginasK6 RiskNilamAnggrianiTambunanAinda não há avaliações
- Atan Baas Sinuhaji Department of Childhood, School of Medicine, University of North Sumatera MedanDocumento8 páginasAtan Baas Sinuhaji Department of Childhood, School of Medicine, University of North Sumatera MedanSyarifah FauziahAinda não há avaliações
- CT Scan Tutorial KoassDocumento40 páginasCT Scan Tutorial KoassenriAinda não há avaliações
- Bisanzo PDFDocumento67 páginasBisanzo PDFenriAinda não há avaliações
- Basic of Thorax Imaging - 10 September 2013 - by Robby HermawanDocumento126 páginasBasic of Thorax Imaging - 10 September 2013 - by Robby HermawanenriAinda não há avaliações
- Ultrasonography: Dr. Achmad Bunyamin SpradDocumento21 páginasUltrasonography: Dr. Achmad Bunyamin SpradenriAinda não há avaliações
- Adaptation To Bright Light (Going From Dark To Light) InvolvesDocumento26 páginasAdaptation To Bright Light (Going From Dark To Light) InvolvesPariksit AnumanthanAinda não há avaliações
- Rts2 - k52 - Nutrisi Gang Respirasi - 2013Documento28 páginasRts2 - k52 - Nutrisi Gang Respirasi - 2013enriAinda não há avaliações
- K.14 Histology of Nasopharynx & PleuraDocumento26 páginasK.14 Histology of Nasopharynx & Pleuraenri0% (1)
- K21 IKA Diarrhoea (Part II)Documento31 páginasK21 IKA Diarrhoea (Part II)enriAinda não há avaliações
- K.3 Mekanika RespirasiDocumento68 páginasK.3 Mekanika RespirasienriAinda não há avaliações
- AmblyopiaDocumento56 páginasAmblyopiaenriAinda não há avaliações
- K.12 Histopatologi Obstruksi ParuDocumento83 páginasK.12 Histopatologi Obstruksi ParuenriAinda não há avaliações
- K.12 Histopatologi Obstruksi ParuDocumento83 páginasK.12 Histopatologi Obstruksi ParuenriAinda não há avaliações
- Introduct&VomitingDocumento47 páginasIntroduct&VomitingenriAinda não há avaliações
- Diarrhoea: Atan Baas SinuhajiDocumento41 páginasDiarrhoea: Atan Baas SinuhajienriAinda não há avaliações
- Diarrhoea: Atan Baas SinuhajiDocumento41 páginasDiarrhoea: Atan Baas SinuhajienriAinda não há avaliações
- Countercurrent MechDocumento27 páginasCountercurrent MechenriAinda não há avaliações
- K14 IPD Dispepsia FungsionalDocumento44 páginasK14 IPD Dispepsia FungsionalenriAinda não há avaliações
- K4 HS Digestive System GlandsDocumento43 páginasK4 HS Digestive System GlandsenriAinda não há avaliações
- Ipd - (Slide Tahun Lalu) IskDocumento49 páginasIpd - (Slide Tahun Lalu) IskenriAinda não há avaliações
- Introduct&VomitingDocumento47 páginasIntroduct&VomitingenriAinda não há avaliações
- (09-10) (IPD) Kelainan Rongga Mulut Dan EsofagusDocumento47 páginas(09-10) (IPD) Kelainan Rongga Mulut Dan EsofagusSures Amoeba RajAinda não há avaliações
- MCQ Tropmed 25 Maret 2010 PublishDocumento27 páginasMCQ Tropmed 25 Maret 2010 PublishDapot Sianipar100% (1)
- Med 12th Feb (1med)Documento39 páginasMed 12th Feb (1med)Naeem AminAinda não há avaliações
- NCM 112 Prefinal LectureDocumento11 páginasNCM 112 Prefinal LectureRheeanne AmilasanAinda não há avaliações
- Pneumococcal Vaccine Timing For AdultsDocumento4 páginasPneumococcal Vaccine Timing For AdultsNur Farhanah Zulkifli100% (1)
- 099 - Small Ruminant HealthDocumento49 páginas099 - Small Ruminant HealthSuraj_Subedi100% (1)
- Biology Passing Material KAYAKA PU COLLEGE KALABURAGIDocumento23 páginasBiology Passing Material KAYAKA PU COLLEGE KALABURAGIRAJAGOPAL93% (15)
- HIV AIDS Knowledge Awareness Perception Amongst First Year Students Medical Nursing PharmacyDocumento4 páginasHIV AIDS Knowledge Awareness Perception Amongst First Year Students Medical Nursing PharmacyAnonymous x8fY69CrnAinda não há avaliações
- Spooky2rifefrequencylist PDFDocumento17 páginasSpooky2rifefrequencylist PDFKevin100% (2)
- Assessing Abdominal Pain in Adults A Rational Cost Effective and Evidence-Based StrategyDocumento20 páginasAssessing Abdominal Pain in Adults A Rational Cost Effective and Evidence-Based StrategyaicitelleticiaAinda não há avaliações
- CirrhosisDocumento10 páginasCirrhosisJénny AnnAinda não há avaliações
- Dr. Limdawati FK Ukm / Rsi 2012Documento45 páginasDr. Limdawati FK Ukm / Rsi 2012Limdawati KweeAinda não há avaliações
- Free Sex Is Very DangerousDocumento1 páginaFree Sex Is Very DangerousNelcy YonnellAinda não há avaliações
- One Health Approach: Saving Lives by Taking ADocumento4 páginasOne Health Approach: Saving Lives by Taking AagneselimAinda não há avaliações
- Diagnosis and Treatment of Fungal Infections - (2015) PDFDocumento298 páginasDiagnosis and Treatment of Fungal Infections - (2015) PDFgaedprietlz25100% (1)
- Microbiology Specimen Collection GuidelinesDocumento16 páginasMicrobiology Specimen Collection Guidelines1DaddictAinda não há avaliações
- 10 1016@j Cmi 2019 12 013Documento25 páginas10 1016@j Cmi 2019 12 013akuAinda não há avaliações
- MAPEH 8 Health - LAS 1 Communicable DiseasesDocumento1 páginaMAPEH 8 Health - LAS 1 Communicable DiseasesYanzy JilhanoAinda não há avaliações
- اسئلة امتحان الهيئة ميكروبيولوجى ومختبرات PDFDocumento18 páginasاسئلة امتحان الهيئة ميكروبيولوجى ومختبرات PDFMaaryMeee RMT0% (1)
- Salmonella EssayDocumento3 páginasSalmonella EssayAlexa LeachAinda não há avaliações
- Acute Upper Airway Obstruction (Power Point)Documento21 páginasAcute Upper Airway Obstruction (Power Point)Sawsan Z. Jwaied100% (2)
- The Novel Coronavirus Disease-2019 (COVID-19) Mechanism of Action, Detection and Recent Therapeutic StrategiesDocumento9 páginasThe Novel Coronavirus Disease-2019 (COVID-19) Mechanism of Action, Detection and Recent Therapeutic Strategiesimamsantos1191Ainda não há avaliações
- Non-Cystic Fibrosis Bronchiectasis: Diagnosis and Management in 21st CenturyDocumento10 páginasNon-Cystic Fibrosis Bronchiectasis: Diagnosis and Management in 21st CenturyIvan VeriswanAinda não há avaliações
- BRS PediatricsDocumento825 páginasBRS PediatricsJsph Ldrn Rly92% (13)
- Babesioza - Teza Doctorat PDFDocumento90 páginasBabesioza - Teza Doctorat PDFAndras AndreescuAinda não há avaliações
- complete wart treatment, two cases of warts treated with isotretinoin, recalcitrant genital warts case reports, Dr Rahul kumar sharma skin specialist ajmer , Dermatologist ajmer, cases of warts, condylomataDocumento3 páginascomplete wart treatment, two cases of warts treated with isotretinoin, recalcitrant genital warts case reports, Dr Rahul kumar sharma skin specialist ajmer , Dermatologist ajmer, cases of warts, condylomataRahul SharmaAinda não há avaliações
- NGU (Varid)Documento11 páginasNGU (Varid)violita22Ainda não há avaliações
- Summary Product Charecteristics: Rabies Vaccine For Human Use, (Vero-Cell) Freeze-Dried (Speeda Vaccine)Documento4 páginasSummary Product Charecteristics: Rabies Vaccine For Human Use, (Vero-Cell) Freeze-Dried (Speeda Vaccine)Ryll Dela CruzAinda não há avaliações
- Case Investigation Forms - Pidsrmop3ed 1Documento16 páginasCase Investigation Forms - Pidsrmop3ed 1RHU Dupax del Sur100% (3)
- Safe Injection Practices ChecklistDocumento8 páginasSafe Injection Practices ChecklistrifkizidnyAinda não há avaliações