Você também pode gostar
- Glute Exercices EbookDocumento22 páginasGlute Exercices EbookHanzel Cornelia100% (1)
- Linck S. R. - Combat Jiu Jitsu PDFDocumento64 páginasLinck S. R. - Combat Jiu Jitsu PDFnautilus81100% (2)
- Neurological ExaminationDocumento13 páginasNeurological Examinationsaveetha purushothamanAinda não há avaliações
- Bobath Approach Concepts and Principles: by DR - Shahid Shabbir DPT, Ms - NMPTDocumento21 páginasBobath Approach Concepts and Principles: by DR - Shahid Shabbir DPT, Ms - NMPTrabia khalid100% (1)
- The Ultimate Push Pull Legs System - 5xDocumento210 páginasThe Ultimate Push Pull Legs System - 5xGilel Drucker67% (3)
- Beginner's GuideDocumento37 páginasBeginner's GuideDawud Muhammad100% (2)
- Occupational Therapy and Life Course Development: A Work Book for Professional PracticeNo EverandOccupational Therapy and Life Course Development: A Work Book for Professional PracticeAinda não há avaliações
- Design of A Hand OrthosisDocumento251 páginasDesign of A Hand OrthosisIsrael BlancoAinda não há avaliações
- OT - Milestone RetypedDocumento6 páginasOT - Milestone RetypedAubrey Vale SagunAinda não há avaliações
- Gym Workout Plan For BeginnersDocumento2 páginasGym Workout Plan For BeginnersrajakprashantAinda não há avaliações
- Nervous System Examination PromptDocumento4 páginasNervous System Examination PromptaeyousefAinda não há avaliações
- FIM or WeeFIM Assessment Scoresheet 2020Documento3 páginasFIM or WeeFIM Assessment Scoresheet 2020Mayco BiasibettiAinda não há avaliações
- Sitbat 16item FinalDocumento6 páginasSitbat 16item FinalMae NocheAinda não há avaliações
- Rehab of Patients With HemiplegiaDocumento2 páginasRehab of Patients With HemiplegiaMilijana D. DelevićAinda não há avaliações
- SCI Acute Care and Rehabilitation PT 2009Documento265 páginasSCI Acute Care and Rehabilitation PT 2009api-3822828Ainda não há avaliações
- Energy Conservation TechniquesDocumento9 páginasEnergy Conservation Techniquesqwas zAinda não há avaliações
- Stroke UE ToolkitDocumento69 páginasStroke UE ToolkitWhitney JosephAinda não há avaliações
- Frame of ReferenceDocumento10 páginasFrame of ReferenceGustavo CabanasAinda não há avaliações
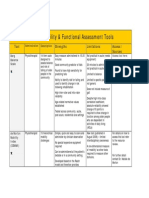
- Mobility and Functional Assessment ToolsDocumento4 páginasMobility and Functional Assessment Toolssonya63265Ainda não há avaliações
- OT Self Care Modified Barthel IndexDocumento4 páginasOT Self Care Modified Barthel Indexlolocy LAinda não há avaliações
- Instrumental Activities Daily Living: Try ThisDocumento11 páginasInstrumental Activities Daily Living: Try ThisbalryoAinda não há avaliações
- Barthel IndexDocumento4 páginasBarthel IndexrlinaoAinda não há avaliações
- Manual TherapyDocumento16 páginasManual TherapylecturioAinda não há avaliações
- Allen Cognitive Level ScreenDocumento9 páginasAllen Cognitive Level ScreenIntan Indah Sari100% (2)
- Orthosisofhandppt 181202162551Documento65 páginasOrthosisofhandppt 181202162551Khageswar SamalAinda não há avaliações
- Barthel ADLsDocumento3 páginasBarthel ADLsGamaliel SeasonAinda não há avaliações
- Low Frequency Currents 1st BPT ChiragDocumento221 páginasLow Frequency Currents 1st BPT ChiragchiragAinda não há avaliações
- Occupational Therapy: SCI, TBI, & CVADocumento35 páginasOccupational Therapy: SCI, TBI, & CVAAnAs Al ArjanAinda não há avaliações
- Derived PositionsDocumento18 páginasDerived PositionsChetan Rathi50% (2)
- Functional Assessment: DR Sonali Soumyashree BPT, MPT (Neurology) Lecturer, GDGUDocumento15 páginasFunctional Assessment: DR Sonali Soumyashree BPT, MPT (Neurology) Lecturer, GDGUSonali Soumyashree100% (2)
- Rubric Mini PracticalDocumento2 páginasRubric Mini PracticalAigen OcampoAinda não há avaliações
- Rheumatology Practice in Occupational Therapy: Promoting Lifestyle ManagementNo EverandRheumatology Practice in Occupational Therapy: Promoting Lifestyle ManagementLynne GoodacreAinda não há avaliações
- OT8 - Thumb Immobilization SplintDocumento4 páginasOT8 - Thumb Immobilization SplintAnnbe Barte100% (1)
- Practice Questions 2Documento61 páginasPractice Questions 2Kilopop Man100% (1)
- Quick DASHDocumento4 páginasQuick DASHKennedy Hindley100% (1)
- Back Biceps WorkoutDocumento2 páginasBack Biceps WorkoutDevendar SharmaAinda não há avaliações
- Occupational Therapy Activities For AdultsDocumento3 páginasOccupational Therapy Activities For AdultsEllee HadesAinda não há avaliações
- Body Dimensions For Apparel Sizing: Standard Terminology Relating ToDocumento13 páginasBody Dimensions For Apparel Sizing: Standard Terminology Relating ToDIEGOAinda não há avaliações
- FIM ManualDocumento24 páginasFIM ManualAnshuman MihirAinda não há avaliações
- App1 Pain Rating ScalesDocumento4 páginasApp1 Pain Rating Scalesthilaga88Ainda não há avaliações
- Wrist Hand OrthosisDocumento3 páginasWrist Hand OrthosisKhageswar SamalAinda não há avaliações
- Part 2: Social Skills Training: RatingDocumento3 páginasPart 2: Social Skills Training: RatingGina GucioAinda não há avaliações
- Lateral Epicondylitis - Tennis Ellbow HandoutDocumento5 páginasLateral Epicondylitis - Tennis Ellbow Handoutgermany23Ainda não há avaliações
- Appendix 8 PDQ39 PDFDocumento3 páginasAppendix 8 PDQ39 PDFdrrselvarajAinda não há avaliações
- Tetraplegia Hand Activity QuestionnaireDocumento20 páginasTetraplegia Hand Activity QuestionnaireISLinkAinda não há avaliações
- Exit Project Workbook Complete Draft 2Documento2 páginasExit Project Workbook Complete Draft 2vladAinda não há avaliações
- Upper Extremity Range of Motion Chart Name: Dob: School Years: Left RightDocumento2 páginasUpper Extremity Range of Motion Chart Name: Dob: School Years: Left RightNatasya SetyamartaAinda não há avaliações
- Spinal Cord Injury Rehabilitation Webinar 2020 PDFDocumento2 páginasSpinal Cord Injury Rehabilitation Webinar 2020 PDFGirijashankar KhuntiaAinda não há avaliações
- INCLEN Diagnostic Tool For Attention Deficit Hyperactive Disorder INDT ADHDDocumento5 páginasINCLEN Diagnostic Tool For Attention Deficit Hyperactive Disorder INDT ADHDNaseeba FaburikageAinda não há avaliações
- Movement Disorders Types - Mayo ClinicDocumento1 páginaMovement Disorders Types - Mayo ClinicdrrajmptnAinda não há avaliações
- The Bobath Concept inDocumento12 páginasThe Bobath Concept inCedricFernandezAinda não há avaliações
- Development Chart For BookletDocumento13 páginasDevelopment Chart For BookletzapelAinda não há avaliações
- EBRSR Handbook Chapter 4 - Upper Extremity Post Stroke - MLDocumento60 páginasEBRSR Handbook Chapter 4 - Upper Extremity Post Stroke - MLanjelikaAinda não há avaliações
- B P O M: Rachial Lexus Utcome EasureDocumento14 páginasB P O M: Rachial Lexus Utcome EasureVirginia Feren FraganzhaAinda não há avaliações
- LABORATORY PRACTICE: Range of Motion WorksheetDocumento12 páginasLABORATORY PRACTICE: Range of Motion WorksheetMike ConnorsAinda não há avaliações
- Cardio Pulmonary AssessmentDocumento8 páginasCardio Pulmonary AssessmentSHAIK SHABEENAAinda não há avaliações
- Muscle Grading and Testing ProceduresDocumento5 páginasMuscle Grading and Testing Proceduresshodhganga100% (1)
- 892 Physiotherapy Management of Paediatric Flat FeetDocumento20 páginas892 Physiotherapy Management of Paediatric Flat FeetCalvina Mizumi100% (1)
- Barthel Index of Activities of Daily LivingDocumento32 páginasBarthel Index of Activities of Daily LivingsimpforaiahAinda não há avaliações
- Sci RehabDocumento45 páginasSci RehabkaushikawebAinda não há avaliações
- Cerebral PalsyDocumento96 páginasCerebral PalsyRahini PaniAinda não há avaliações
- Gait in Children With Cerebral PalsyDocumento5 páginasGait in Children With Cerebral PalsyvarahamihirAinda não há avaliações
- Motion Tested/ Endfeel Position/ Normal Range AxisDocumento6 páginasMotion Tested/ Endfeel Position/ Normal Range AxisMarji BerkmanAinda não há avaliações
- Immobilization Protocol For Extensor Tendon RepairDocumento2 páginasImmobilization Protocol For Extensor Tendon RepairFatin NawarahAinda não há avaliações
- Post Stroke Functional Exercises For RehabilitationDocumento37 páginasPost Stroke Functional Exercises For Rehabilitationjoel_simon_23100% (1)
- Roods ApproachDocumento33 páginasRoods ApproachCedricFernandez100% (1)
- Early Intervention - ErgonomicsDocumento5 páginasEarly Intervention - ErgonomicsKhatri NasrullahAinda não há avaliações
- Tinetti Assessment BalanceDocumento3 páginasTinetti Assessment BalanceAlexandra DeacAinda não há avaliações
- GMFM (GMFM-66 & GMFM-88) User's Manual, 2nd editionNo EverandGMFM (GMFM-66 & GMFM-88) User's Manual, 2nd editionNota: 1 de 5 estrelas1/5 (1)
- Neurological Assessment in the First Two Years of LifeNo EverandNeurological Assessment in the First Two Years of LifeGiovanni CioniAinda não há avaliações
- Psychogenic Aspects of ExerciseDocumento29 páginasPsychogenic Aspects of Exercisechirag100% (1)
- Principles of MotionDocumento29 páginasPrinciples of MotionchiragAinda não há avaliações
- Disaster ManagementDocumento24 páginasDisaster ManagementchiragAinda não há avaliações
- Soleus - PhysiopediaDocumento6 páginasSoleus - PhysiopediaVahid AtaeiAinda não há avaliações
- Varmam RX For Musculo Skeletal DisorderDocumento5 páginasVarmam RX For Musculo Skeletal DisorderYoga Naayak100% (1)
- Closed Reduction of Posterior Hip DislocationDocumento4 páginasClosed Reduction of Posterior Hip DislocationHannah JuanitaAinda não há avaliações
- Pursuit MobilityDocumento27 páginasPursuit MobilityAvinash PulickalAinda não há avaliações
- 68 Text 362 1 10 20220624Documento7 páginas68 Text 362 1 10 20220624YesicaAinda não há avaliações
- CHAPTER 7 The Muscular SystemDocumento6 páginasCHAPTER 7 The Muscular SystemRenson S. HermoginoAinda não há avaliações
- Rehabilitation Guidelines For Posterior Cruciate Ligament ReconstructionDocumento6 páginasRehabilitation Guidelines For Posterior Cruciate Ligament ReconstructionMono MostafaAinda não há avaliações
- Posterior Malleolar Fractures: A Critical Analysis ReviewDocumento17 páginasPosterior Malleolar Fractures: A Critical Analysis ReviewJohn Sebastian ValenciaAinda não há avaliações
- Cubital FossaDocumento12 páginasCubital FossaIjaz KhanAinda não há avaliações
- Elderly Program RealDocumento5 páginasElderly Program RealDebianAinda não há avaliações
- Rivero 1991. New Ecuadorean Colostethus (Amphibia, Dendrobatidae) in The Collection of The National Museum of Natural History, Smithsonian InstitutionDocumento16 páginasRivero 1991. New Ecuadorean Colostethus (Amphibia, Dendrobatidae) in The Collection of The National Museum of Natural History, Smithsonian InstitutionNicole AcosVas0% (1)
- 90min Push Pull LegsDocumento11 páginas90min Push Pull LegsHariprasaadAinda não há avaliações
- Harbinger - Fitness Guide CablesDocumento2 páginasHarbinger - Fitness Guide Cablesedwin69roAinda não há avaliações
- Detailed - Robotic-Arm Assisted MAKO SurgeryDocumento25 páginasDetailed - Robotic-Arm Assisted MAKO Surgeryswastik baratAinda não há avaliações
- Musculoskeletal History: Basic InfoDocumento10 páginasMusculoskeletal History: Basic InfoTom MallinsonAinda não há avaliações
- Medial Collateral Ligament InjuriesDocumento14 páginasMedial Collateral Ligament InjuriesosamadrAinda não há avaliações
- Elbow Fractures: Distal Humerus: The American Society For Surgery of The Hand.)Documento15 páginasElbow Fractures: Distal Humerus: The American Society For Surgery of The Hand.)Radu UrcanAinda não há avaliações
- Anatomy of The Hip: Principles of Orthopaedic and Trauma Care December 2008 Faculty of Health & Life Sciences UWEDocumento34 páginasAnatomy of The Hip: Principles of Orthopaedic and Trauma Care December 2008 Faculty of Health & Life Sciences UWESivabharathi Sivanandam100% (1)
- 8th Class Disability Evaluation-UpperlimbDocumento34 páginas8th Class Disability Evaluation-UpperlimbRashmi SheelvantAinda não há avaliações
- Session 1 Hip and PelvisDocumento62 páginasSession 1 Hip and PelvisNixon BiasAinda não há avaliações