Você também pode gostar
- Dental Anatomy and PhysiologyDocumento36 páginasDental Anatomy and PhysiologyCpt.WnchstrAinda não há avaliações
- IFDEA Dental Anatomy Educational Teaching ResourceDocumento38 páginasIFDEA Dental Anatomy Educational Teaching ResourcelienhuongahAinda não há avaliações
- Oral AnatomyDocumento25 páginasOral AnatomyFlip CartAinda não há avaliações
- Anatomi Gigi Geligi by TinaDocumento44 páginasAnatomi Gigi Geligi by TinaTegAinda não há avaliações
- Dental AnatomyDocumento24 páginasDental Anatomysιηηεя ðԲ ťḩë ḩëL·L·Ainda não há avaliações
- Dentistry 2012 E.CDocumento445 páginasDentistry 2012 E.Csintayhu nigatuAinda não há avaliações
- Dental Anatomy & Physiology: Lokender Yadav Sr-Manager Talent Development Unicorn Denmart LimitedDocumento37 páginasDental Anatomy & Physiology: Lokender Yadav Sr-Manager Talent Development Unicorn Denmart LimitedLokender Yadav100% (1)
- Introduction To Dentistry and Dental Terminology: English For Dental NurseDocumento74 páginasIntroduction To Dentistry and Dental Terminology: English For Dental NurseREFTA DEVI100% (1)
- Parts of The ToothDocumento22 páginasParts of The Toothd389Ainda não há avaliações
- Fornemc 15111Documento98 páginasFornemc 15111Vanshika SethiAinda não há avaliações
- Teeth, Vessels and Nerves of Oral CavityDocumento86 páginasTeeth, Vessels and Nerves of Oral Cavityk20221163Ainda não há avaliações
- Basic Guide To Dental InstrumentsDocumento7 páginasBasic Guide To Dental Instrumentssinofrisa31Ainda não há avaliações
- Lecture 1 Powerpoint VersionDocumento40 páginasLecture 1 Powerpoint VersionChun Ming IpAinda não há avaliações
- Dental Anatomy 1Documento33 páginasDental Anatomy 1dehaa100% (1)
- Terminology Used To Describe The Tissues of A Tooth: DR - Yad Raouf BDS, Efb, MrcsedDocumento20 páginasTerminology Used To Describe The Tissues of A Tooth: DR - Yad Raouf BDS, Efb, MrcsedRabarAinda não há avaliações
- Introduction To Oral HistologyDocumento30 páginasIntroduction To Oral HistologyShalini NairAinda não há avaliações
- IFDEA Dental Anatomy Educational Teaching ResourceDocumento38 páginasIFDEA Dental Anatomy Educational Teaching ResourceaerowongAinda não há avaliações
- Dental Anatomy & Physiology: Physiology, Etiology, Epidemiology, Diagnosis, and TreatmentDocumento38 páginasDental Anatomy & Physiology: Physiology, Etiology, Epidemiology, Diagnosis, and TreatmentdrsunjithAinda não há avaliações
- Morphology II - Lecture 1, Dental StructuresDocumento22 páginasMorphology II - Lecture 1, Dental Structuressven.kruetzfeldtAinda não há avaliações
- 2 - Human Dentition IntroDocumento71 páginas2 - Human Dentition IntroozyiamandsAinda não há avaliações
- Chapter 4 - Dental Anatomy (Essentials of Dental Assisting)Documento28 páginasChapter 4 - Dental Anatomy (Essentials of Dental Assisting)mussanteAinda não há avaliações
- Structure of Tooth 2014 ID TopicsDocumento24 páginasStructure of Tooth 2014 ID TopicsIsdianaAinda não há avaliações
- Structure of Tooth m121Documento13 páginasStructure of Tooth m121amirhossein vaeziAinda não há avaliações
- Radiological Anatomy of The Facial Massive Variations in Size, Number and Shape of TeethDocumento143 páginasRadiological Anatomy of The Facial Massive Variations in Size, Number and Shape of TeethRodicaAinda não há avaliações
- Prelegere Anom Dent ENG+anomaliDocumento143 páginasPrelegere Anom Dent ENG+anomaliMaria GorodencoAinda não há avaliações
- Dental Anatomy & PhysiologyDocumento38 páginasDental Anatomy & PhysiologynumbnessAinda não há avaliações
- Oral Cavity: ObjectivesDocumento24 páginasOral Cavity: ObjectivestazeAinda não há avaliações
- Oral Structures and Types of Teeth: Ms. Zain Malkawi, MSDHDocumento28 páginasOral Structures and Types of Teeth: Ms. Zain Malkawi, MSDHAHMED EZZATAinda não há avaliações
- Tooth AnatomyDocumento31 páginasTooth Anatomydhea wirantiAinda não há avaliações
- Kuliah Gigi Dan MulutDocumento75 páginasKuliah Gigi Dan MulutWendz BouvierAinda não há avaliações
- Tooth Morphology Histology Development PDFDocumento55 páginasTooth Morphology Histology Development PDFElena BordeianuAinda não há avaliações
- Development of TeethDocumento20 páginasDevelopment of TeethSubhashini RajshekarAinda não há avaliações
- Dentin Oral Histology and PhysiologyDocumento72 páginasDentin Oral Histology and PhysiologyJamal NaimAinda não há avaliações
- LectureDocumento1 páginaLectureSariya KabbaneeeAinda não há avaliações
- Development of TeethDocumento20 páginasDevelopment of TeethMehri Aisha ShanavasAinda não há avaliações
- Presentación Diapositivas Negocio Catering Comida Ilustrativo Verde y BeigeDocumento12 páginasPresentación Diapositivas Negocio Catering Comida Ilustrativo Verde y BeigeIsabela HidalgoAinda não há avaliações
- TeethDocumento3 páginasTeethSabita SinghAinda não há avaliações
- Dental Anatomy: Đỗ Ngọc Thanh Trúc - 20RHM1Documento9 páginasDental Anatomy: Đỗ Ngọc Thanh Trúc - 20RHM1Dũng NguyễnAinda não há avaliações
- Significance of Dental Anatomy, Histology, Physiology, and Occlusion (L1)Documento54 páginasSignificance of Dental Anatomy, Histology, Physiology, and Occlusion (L1)Jarrah LumpayAinda não há avaliações
- 1 IntroductionDocumento38 páginas1 IntroductionMimo HemadAinda não há avaliações
- An Overview of Dental AnatomyDocumento16 páginasAn Overview of Dental Anatomyaimazaika1234Ainda não há avaliações
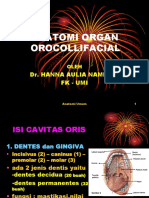
- Anatomi Organ Orocollifacial: Dr. Hanna Aulia Namirah FK - UmiDocumento93 páginasAnatomi Organ Orocollifacial: Dr. Hanna Aulia Namirah FK - Umiselly silla saktiAinda não há avaliações
- Taeb 487 Tooth StructureDocumento14 páginasTaeb 487 Tooth StructuremohammedAinda não há avaliações
- Dentistry FinalDocumento68 páginasDentistry Finaladwait marhatta100% (1)
- Tooth Structure 9075Documento2 páginasTooth Structure 9075Andreea CojocariAinda não há avaliações
- Car 2Documento68 páginasCar 2Diana ConcepcionAinda não há avaliações
- Tooth DevelopmentDocumento20 páginasTooth DevelopmentArslan Jokhio0% (1)
- Oral Histology ProjectionDocumento92 páginasOral Histology ProjectionMOHAMMEDAinda não há avaliações
- Tooth Morphology Basics: Howard Chi, D.M.DDocumento79 páginasTooth Morphology Basics: Howard Chi, D.M.DMihaela Vasiliu0% (1)
- Dentin: V.Nivedha First Year MDS 14.07.2017Documento118 páginasDentin: V.Nivedha First Year MDS 14.07.2017Khalid Lafi100% (1)
- Tiếng Anh RHMDocumento11 páginasTiếng Anh RHMĐá CuộiAinda não há avaliações
- Comprehensive Dental Notes For MBBS - LohaniDocumento68 páginasComprehensive Dental Notes For MBBS - LohaniPratik100% (1)
- Tooth AnatomyDocumento34 páginasTooth Anatomyezoafaneh0Ainda não há avaliações
- Oral Histology SlidesDocumento60 páginasOral Histology SlidesRan And SanAinda não há avaliações
- Teeth NotesDocumento3 páginasTeeth NotesTamisha JacobsAinda não há avaliações
- Final PDLDocumento100 páginasFinal PDLDrRahat SaleemAinda não há avaliações
- COOKERY 9 Quarter 4 LAS Number 2Documento3 páginasCOOKERY 9 Quarter 4 LAS Number 2Rhea Alo67% (3)
- A Christmas Crossword PuzzleDocumento3 páginasA Christmas Crossword Puzzlemakbuddy50% (2)
- The Hungry Empire - How Britain's Quest For Food Shaped The Modern WorldDocumento3 páginasThe Hungry Empire - How Britain's Quest For Food Shaped The Modern WorldHellen CristanchoAinda não há avaliações
- Like Dislike Questionnaire Updated Sept 2013Documento6 páginasLike Dislike Questionnaire Updated Sept 2013api-235760990Ainda não há avaliações
- Meet OUR Ambas Sadors: Ramon PerezDocumento5 páginasMeet OUR Ambas Sadors: Ramon PerezAntonisMavridisAinda não há avaliações
- MAPEHTHIRDEXAMDocumento7 páginasMAPEHTHIRDEXAMjay meilyAinda não há avaliações
- FEEL THE LEAN EBOOK Lonijane PDFDocumento192 páginasFEEL THE LEAN EBOOK Lonijane PDFAmethyst Carey100% (5)
- Dinner MenuDocumento1 páginaDinner MenueatlocalmenusAinda não há avaliações
- GAF686 - Recipe BookDocumento68 páginasGAF686 - Recipe Bookerwin_betancourt_2Ainda não há avaliações
- Materi Bahasa Inggris Kelas 3 SDDocumento13 páginasMateri Bahasa Inggris Kelas 3 SDicaAinda não há avaliações
- Science 4 - q1 - Module 4of6 - Changes That Mareials Undergowhen Mixed With Other Materials - v2Documento20 páginasScience 4 - q1 - Module 4of6 - Changes That Mareials Undergowhen Mixed With Other Materials - v2Mary Ann BernalesAinda não há avaliações
- Managing Philanthropy - BCF Covid Special Report 2020Documento24 páginasManaging Philanthropy - BCF Covid Special Report 2020BernewsAdminAinda não há avaliações
- LimeDocumento19 páginasLimeapi-3737745100% (1)
- Qse Adv TG 09 Exam Answer KeyDocumento4 páginasQse Adv TG 09 Exam Answer KeyCristian GutierrezAinda não há avaliações
- Compact Dry SL (For Salmonella) : 40/240/920 Plates Id No. 1002973/1002938/1002940Documento1 páginaCompact Dry SL (For Salmonella) : 40/240/920 Plates Id No. 1002973/1002938/1002940Wendy Núñez BedollaAinda não há avaliações
- Science Year 5 TestDocumento21 páginasScience Year 5 TestSithar DeviAinda não há avaliações
- Sensory ImageryDocumento4 páginasSensory ImageryMaristela RamosAinda não há avaliações
- Mayr Franz. Zulu ProverbsDocumento10 páginasMayr Franz. Zulu ProverbsAzarias VilanculosAinda não há avaliações
- PENGARUH PEMBERIAN NAUNGAN DAN PUPUK ORGANIK CAIR TERHADAP PERTUMBUHAN DAN PRODUKSI TANAMAN STROBERI (Fragaria SP.) DI DATARAN RENDAHDocumento13 páginasPENGARUH PEMBERIAN NAUNGAN DAN PUPUK ORGANIK CAIR TERHADAP PERTUMBUHAN DAN PRODUKSI TANAMAN STROBERI (Fragaria SP.) DI DATARAN RENDAHrudy hery syahfutroAinda não há avaliações
- Toxoplasmosis BrochureDocumento2 páginasToxoplasmosis Brochurethecatisgay100% (1)
- MezzeDocumento10 páginasMezzelizspbrazilAinda não há avaliações
- Constructing Markets For AgroecologyDocumento214 páginasConstructing Markets For AgroecologydutvaAinda não há avaliações
- Second Term Examination Grade Three 2020-2021Documento14 páginasSecond Term Examination Grade Three 2020-2021Enuma JamesAinda não há avaliações
- Notes On Book - 1Documento57 páginasNotes On Book - 1Uzair AmjadAinda não há avaliações
- HSSC PAPER 21 (16) - WatermarkDocumento27 páginasHSSC PAPER 21 (16) - WatermarkJitender TanwarAinda não há avaliações
- Soal Bahasa Inggris Semester Ganjil Kelas XiDocumento6 páginasSoal Bahasa Inggris Semester Ganjil Kelas XiAchsien100% (1)
- SWOT Analysis of Pepsi CompanyDocumento7 páginasSWOT Analysis of Pepsi CompanyUrmi Mehta100% (1)
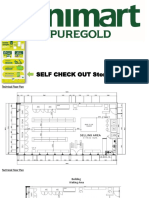
- Puregold Minimart Requirements For StudentsDocumento13 páginasPuregold Minimart Requirements For StudentsRhynelle TolentinoAinda não há avaliações
- Kartu Soal Asas B.inggris Kelas ViiDocumento21 páginasKartu Soal Asas B.inggris Kelas ViiArin Nurul NingtyasAinda não há avaliações
- Grade 8Documento5 páginasGrade 8Geneva Faye Lirazan MendozaAinda não há avaliações