Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Amina PrimerDocumento13 páginasAmina PrimerYoan YasrilAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Uji 1 2Documento2 páginasUji 1 2Yoan YasrilAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Jurnal 8Documento4 páginasJurnal 8Yoan YasrilAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- KWN 2013Documento3 páginasKWN 2013Yoan YasrilAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Uji 1Documento2 páginasUji 1Yoan YasrilAinda não há avaliações
- PneumonitisDocumento10 páginasPneumonitisYoan YasrilAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Respiration BiologyDocumento25 páginasRespiration BiologyYoan YasrilAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- PneumonitisDocumento10 páginasPneumonitisYoan YasrilAinda não há avaliações
- Kelompok 5Documento80 páginasKelompok 5Yoan YasrilAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- Pharmaceutical MicrobiologyDocumento2 páginasPharmaceutical MicrobiologyYoan YasrilAinda não há avaliações
- Self Eficacy Kepribadian Dan LODocumento18 páginasSelf Eficacy Kepribadian Dan LOYoan YasrilAinda não há avaliações
- 1 s2.0 S1877042813053287 MainDocumento7 páginas1 s2.0 S1877042813053287 MainYoan YasrilAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Crospovidone Ad 2Documento7 páginasCrospovidone Ad 2Yoan YasrilAinda não há avaliações
- Day 1-5 James Butler FinalDocumento22 páginasDay 1-5 James Butler FinalPedro MaiaAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Dapus Umum LengkapDocumento6 páginasDapus Umum LengkapDhewiantyAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Sma Drug Pipeline: Basic Research Seed IdeasDocumento1 páginaSma Drug Pipeline: Basic Research Seed IdeassvaleravnAinda não há avaliações
- Paper Tablets Lab ActivityDocumento4 páginasPaper Tablets Lab ActivityRosales Gemson Lyster100% (2)
- Evaluation of Price Disparity Among Generic Medicines in IndiaDocumento3 páginasEvaluation of Price Disparity Among Generic Medicines in Indiadada patilAinda não há avaliações
- Antiretroviral Therapy (ART) : When, How To Start HAART and Combination TherapiesDocumento36 páginasAntiretroviral Therapy (ART) : When, How To Start HAART and Combination TherapiesMwanja MosesAinda não há avaliações
- ACFrOgDMeWktqztT - MCQzkrLPX1KtTJlmgfBDZ3R 9g4LpaMwxB5l7h6XTsHdSVEF4WNzE7t8UEpR8stZ37NKJ4 sMKGVlq4FDCTJtFdAp8M3V0XWnwkMh7I1TDvypADocumento7 páginasACFrOgDMeWktqztT - MCQzkrLPX1KtTJlmgfBDZ3R 9g4LpaMwxB5l7h6XTsHdSVEF4WNzE7t8UEpR8stZ37NKJ4 sMKGVlq4FDCTJtFdAp8M3V0XWnwkMh7I1TDvypAdsnbkprasanthAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Vet Pharmacology BasicsDocumento75 páginasVet Pharmacology Basicsibriane eveAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- TDMDocumento192 páginasTDMyeeteng0819Ainda não há avaliações
- Product MataDocumento8 páginasProduct MataBinsar Randy DvmAinda não há avaliações
- Eli Lilly Case (MM Presentation)Documento43 páginasEli Lilly Case (MM Presentation)vinaytoshchoudharyAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Primo GelDocumento10 páginasPrimo Gelandika adikaraAinda não há avaliações
- Geriatric Pharmacotherapy: Understanding Age-Related Changes to Optimize Drug TherapyDocumento48 páginasGeriatric Pharmacotherapy: Understanding Age-Related Changes to Optimize Drug Therapywalt65Ainda não há avaliações
- Investigational New Drug Application (IND)Documento27 páginasInvestigational New Drug Application (IND)Pharmacology MnemonicsAinda não há avaliações
- "SUN TEN" PHARMACEUTICAL CO., LTD The Transformation of Company (Within 1000 Wordks)Documento5 páginas"SUN TEN" PHARMACEUTICAL CO., LTD The Transformation of Company (Within 1000 Wordks)SaOdah GurningAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Pharmacy Profession in Nepal Has History Only of About 50 Years BackDocumento4 páginasPharmacy Profession in Nepal Has History Only of About 50 Years BackSushant Aryal100% (1)
- Agitation, Diaphoresis, Diarrhea, Fever, Hyperreflexia, Incoordination, Confusion, Myoclonus, Shivering or TremorDocumento2 páginasAgitation, Diaphoresis, Diarrhea, Fever, Hyperreflexia, Incoordination, Confusion, Myoclonus, Shivering or TremorMark Darren MiguelAinda não há avaliações
- Nearest Pharmacy Delivery ServiceDocumento5 páginasNearest Pharmacy Delivery ServiceJayanath SamarasingheAinda não há avaliações
- Ana HJKDocumento2 páginasAna HJKbesoAinda não há avaliações
- Bài tập viết lại câu - Ngoại ngữ 4Documento3 páginasBài tập viết lại câu - Ngoại ngữ 4Nguyễn HàAinda não há avaliações
- Vise Cene LekovaDocumento29 páginasVise Cene LekovaDanijela RakicAinda não há avaliações
- Chapter 50 Principles of PharmacologyDocumento47 páginasChapter 50 Principles of PharmacologyTee WoodAinda não há avaliações
- Test Bank For Integrated Cardiopulmonary Pharmacology 3rd Edition ColbertDocumento6 páginasTest Bank For Integrated Cardiopulmonary Pharmacology 3rd Edition Colbertorlaedithhyi5xAinda não há avaliações
- MCQ AduaDocumento4 páginasMCQ AduaSummer Mamun100% (1)
- Digoxin Dosing: o o o o oDocumento4 páginasDigoxin Dosing: o o o o oLindaAinda não há avaliações
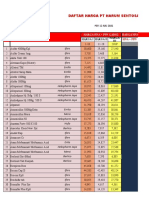
- NO Nama Obat: Daftar Harga PT Harum SentosaDocumento32 páginasNO Nama Obat: Daftar Harga PT Harum SentosaFahmi HaryadinAinda não há avaliações
- Pharmaceuti Ca Science 2019Documento32 páginasPharmaceuti Ca Science 2019Alah Bacot.Ainda não há avaliações
- Pharmacokinetics and Bioavailability of Florfenicol Following Intravenous, Intramuscular and Oral Administrations in RabbitsDocumento10 páginasPharmacokinetics and Bioavailability of Florfenicol Following Intravenous, Intramuscular and Oral Administrations in RabbitsJohanna Valentina López CortesAinda não há avaliações
- Anticoagulation Guidelines For Neuraxial Procedures: Anticoagulants, InjectableDocumento4 páginasAnticoagulation Guidelines For Neuraxial Procedures: Anticoagulants, InjectablepaulaAinda não há avaliações
- Antiviral drugs and their propertiesDocumento1 páginaAntiviral drugs and their propertiesGustika AzharAinda não há avaliações