Você também pode gostar
- Hyponatremia (Emphasis On SIADH) : DR Adeyemo A. ODocumento57 páginasHyponatremia (Emphasis On SIADH) : DR Adeyemo A. OAdeyemo AyoadeAinda não há avaliações
- Neuroimaging and DNA Profiling New AvenuesDocumento52 páginasNeuroimaging and DNA Profiling New AvenuesDr-Ajay TripathiAinda não há avaliações
- HyponatraemiaDocumento16 páginasHyponatraemiaRaluca LeucaAinda não há avaliações
- HyponatremiaDocumento6 páginasHyponatremiaJaymart Saclolo CostillasAinda não há avaliações
- Hyponatremia: BY: Dr. Sammon K TareenDocumento35 páginasHyponatremia: BY: Dr. Sammon K TareenSammon TareenAinda não há avaliações
- The Hyponatremic Patient: A Systematic Approach To Laboratory DiagnosisDocumento7 páginasThe Hyponatremic Patient: A Systematic Approach To Laboratory DiagnosisJuen LohAinda não há avaliações
- Hyponatremia: Causes, Evaluation & TreatmentDocumento20 páginasHyponatremia: Causes, Evaluation & TreatmentmanjaruAinda não há avaliações
- Diabetes Insipidus & Syndrome of Inappropiate Antidiuretic HormoneDocumento16 páginasDiabetes Insipidus & Syndrome of Inappropiate Antidiuretic HormoneStephanie RiveraAinda não há avaliações
- Final Version of PropagandaDocumento41 páginasFinal Version of PropagandaZara IftikharAinda não há avaliações
- Electrolyte DisordersDocumento10 páginasElectrolyte DisordersSlavicaAinda não há avaliações
- Sodium & Water Disorders: Understanding Hyponatremia and HypernatremiaDocumento39 páginasSodium & Water Disorders: Understanding Hyponatremia and HypernatremiaManhal A AbdulkaderAinda não há avaliações
- How I Approach Hyponatraemia: CME EndocrinologyDocumento6 páginasHow I Approach Hyponatraemia: CME EndocrinologyFernando Re TaAinda não há avaliações
- SIADH (Syndrome of Inapproperiate Antidiuretic Hormone Secretion)Documento11 páginasSIADH (Syndrome of Inapproperiate Antidiuretic Hormone Secretion)itsmesubu100% (2)
- Fluid & Electrolyte Management & Acid Base Disorders: Alice Augustin Amina S Anagha P RDocumento47 páginasFluid & Electrolyte Management & Acid Base Disorders: Alice Augustin Amina S Anagha P RAsif AbbasAinda não há avaliações
- A Systematic Approach To The Hyponatremic Patient: Iva Ratkoviê-Gusiê, Petar Kes And Vanja Baπiê-KesDocumento10 páginasA Systematic Approach To The Hyponatremic Patient: Iva Ratkoviê-Gusiê, Petar Kes And Vanja Baπiê-KesTio Prima SAinda não há avaliações
- Plications of HemodialysisDocumento30 páginasPlications of HemodialysisAISHWARYA T DAinda não há avaliações
- Diabetes Insipidus, Siadh and Cerebral Salt-WastingDocumento33 páginasDiabetes Insipidus, Siadh and Cerebral Salt-WastingEuphrasiaAinda não há avaliações
- Hypokalaemia and HyperkalaemiaDocumento39 páginasHypokalaemia and HyperkalaemiaRZ NgAinda não há avaliações
- XAVIER UNIVERSITY – ATENEO DE CAGAYAN COLLEGE OF NURSING CONCEPT MAP: HYPONATREMIADocumento9 páginasXAVIER UNIVERSITY – ATENEO DE CAGAYAN COLLEGE OF NURSING CONCEPT MAP: HYPONATREMIAElleAinda não há avaliações
- HiponatremiaDocumento8 páginasHiponatremiaMeidistya Ayu MardhianiAinda não há avaliações
- M5 - Electrolyte AbnormalitiesDocumento44 páginasM5 - Electrolyte AbnormalitiesVishal KumarAinda não há avaliações
- Pathophysiology and Etiology of The Syndrome of Inappropriate Antidiuretic Hormone Secretion (Siadh)Documento24 páginasPathophysiology and Etiology of The Syndrome of Inappropriate Antidiuretic Hormone Secretion (Siadh)Urgencias E.S.E Coromoro - Centro salud CinceladaAinda não há avaliações
- Guidelines For The Management of HyponatraemiaDocumento8 páginasGuidelines For The Management of HyponatraemiaMuhammad Amiro RasheeqAinda não há avaliações
- Approach To Fluid and Electrolyte Disorders and Acid-Base ProblemsDocumento19 páginasApproach To Fluid and Electrolyte Disorders and Acid-Base ProblemsHigh EducationAinda não há avaliações
- Manajemen Anestesi Pada Uremic SyndromeDocumento27 páginasManajemen Anestesi Pada Uremic SyndromeAdi Nugroho MelyanaAinda não há avaliações
- Fluid and Electrolytes Assignment 1. What Are The Different Processes of Body Fluid and Solutes Movement? and Give at Least 2 Examples EachDocumento8 páginasFluid and Electrolytes Assignment 1. What Are The Different Processes of Body Fluid and Solutes Movement? and Give at Least 2 Examples EachAngelicaAinda não há avaliações
- Fluid and Electrolytes Assignment 1. What Are The Different Processes of Body Fluid and Solutes Movement? and Give at Least 2 Examples EachDocumento8 páginasFluid and Electrolytes Assignment 1. What Are The Different Processes of Body Fluid and Solutes Movement? and Give at Least 2 Examples EachAngelicaAinda não há avaliações
- NCM 3114 Electrolyte Imbalance-2Documento21 páginasNCM 3114 Electrolyte Imbalance-2Nicole Sherry M. CHEEAinda não há avaliações
- Electrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesDocumento44 páginasElectrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesNinaAinda não há avaliações
- Hyponatremia: Q: Discuss Hyponatremia in Clinical PracticeDocumento7 páginasHyponatremia: Q: Discuss Hyponatremia in Clinical PracticemyqueenleoAinda não há avaliações
- Surgery YbDocumento67 páginasSurgery YbTamirat geletaAinda não há avaliações
- Guideline, Management of HypernatremiaDocumento9 páginasGuideline, Management of HypernatremiaLia Safitri Leloly100% (1)
- By DR Madhusudan C Associate Professor Department of MedicineDocumento39 páginasBy DR Madhusudan C Associate Professor Department of MedicineTeena ChandranAinda não há avaliações
- ENDO... ElectrolyteDocumento44 páginasENDO... ElectrolyteOmar AbdillahiAinda não há avaliações
- Chapter 16: Disorders of Serum Sodium Concentration in The Elderly PatientDocumento6 páginasChapter 16: Disorders of Serum Sodium Concentration in The Elderly PatientYantimuliawatiAinda não há avaliações
- Causes of Hyponatremia in AdultsDocumento18 páginasCauses of Hyponatremia in AdultsAndro Franco Florio CatalánAinda não há avaliações
- AldosteronismDocumento48 páginasAldosteronismMiguel Cuevas DolotAinda não há avaliações
- HyponatremiaDocumento21 páginasHyponatremiaselma100% (1)
- Chronic Kidney DiseaseDocumento6 páginasChronic Kidney Diseaseashi leginAinda não há avaliações
- Lab Data InterpretationDocumento38 páginasLab Data Interpretationraziajaffery14Ainda não há avaliações
- Fluids and Electrolytes and Acid Base PhysiologyDocumento64 páginasFluids and Electrolytes and Acid Base PhysiologyJesserene Mangulad SorianoAinda não há avaliações
- RANASINGHE Fluid Electrolyte and Acid Base PhysiologyDocumento45 páginasRANASINGHE Fluid Electrolyte and Acid Base PhysiologyDagimAinda não há avaliações
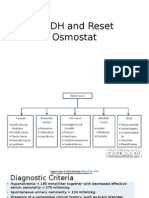
- SIADH and Reset OsmostatDocumento7 páginasSIADH and Reset Osmostatsaleema11Ainda não há avaliações
- Page 1 of 6Documento6 páginasPage 1 of 6Karissa MagaruAinda não há avaliações
- Group 1 SiadhDocumento22 páginasGroup 1 SiadhFuzna DahliaAinda não há avaliações
- MINI ReviewDocumento10 páginasMINI ReviewShamila KaruthuAinda não há avaliações
- Indications of Dialysis in Acute Renal Failure (ARF)Documento3 páginasIndications of Dialysis in Acute Renal Failure (ARF)Tariku GelesheAinda não há avaliações
- Disorders of Carbohydrate Metabolism.: Abdelmoniem Saeed Mohammed Er SpecialistDocumento49 páginasDisorders of Carbohydrate Metabolism.: Abdelmoniem Saeed Mohammed Er SpecialistYousef Al-AmeenAinda não há avaliações
- Defining SIADHDocumento2 páginasDefining SIADHJohan El-Hakim Siregar100% (1)
- Hyponatremia Guide: Causes, Diagnosis & TreatmentDocumento2 páginasHyponatremia Guide: Causes, Diagnosis & TreatmentAlimu SowAinda não há avaliações
- Fispatologjia e CreegullimeveDocumento16 páginasFispatologjia e CreegullimeveArmar MendoAinda não há avaliações
- Electrolyte Imbalance: Sodium: Submitted By: Milosantos, John Francis D. Tuibeo, Ma. Arlyn P. Yu, Aldrin Anthony LDocumento6 páginasElectrolyte Imbalance: Sodium: Submitted By: Milosantos, John Francis D. Tuibeo, Ma. Arlyn P. Yu, Aldrin Anthony Lnospekiko21Ainda não há avaliações
- Understanding Hyponatremia: Causes, Symptoms and TreatmentDocumento44 páginasUnderstanding Hyponatremia: Causes, Symptoms and TreatmentSteven Godelman100% (3)
- Acute Renal Failure Nursing Care PlanDocumento15 páginasAcute Renal Failure Nursing Care PlanRanusha AnushaAinda não há avaliações
- 12-1 Diabetic Emergencies-HHS PDFDocumento12 páginas12-1 Diabetic Emergencies-HHS PDFOana DumitruAinda não há avaliações
- Understanding SIADH: Causes, Symptoms and TreatmentDocumento20 páginasUnderstanding SIADH: Causes, Symptoms and TreatmentArul MAinda não há avaliações
- Siadh & Hyponatremia: Dr. Kushal Markanday MDDocumento67 páginasSiadh & Hyponatremia: Dr. Kushal Markanday MD966342100% (1)
- Electrolyte DisturbanceDocumento57 páginasElectrolyte DisturbanceMrrAinda não há avaliações
- PBL 1Documento111 páginasPBL 1fahmi rosyadiAinda não há avaliações
- Nursing: Lab Values: a QuickStudy Laminated 6-Page Reference GuideNo EverandNursing: Lab Values: a QuickStudy Laminated 6-Page Reference GuideAinda não há avaliações
- Short Breath History NotesDocumento41 páginasShort Breath History NotesAhmed AbdelgelilAinda não há avaliações
- IMPO Info For PACES (DR Shiny Moon)Documento3 páginasIMPO Info For PACES (DR Shiny Moon)Ahmed AbdelgelilAinda não há avaliações
- Identify Vein, Artery, Disc, Optic Cup, FoveaDocumento30 páginasIdentify Vein, Artery, Disc, Optic Cup, FoveaAhmed AbdelgelilAinda não há avaliações
- Acute Confusional State ManagementDocumento18 páginasAcute Confusional State ManagementAhmed AbdelgelilAinda não há avaliações
- 4 Tips For Passing PACES: PreparationDocumento10 páginas4 Tips For Passing PACES: PreparationAhmed AbdelgelilAinda não há avaliações
- My Masterclass Exam #59765: About Products Buy Institutions Exam Demo Video Demo Contact Us FAQ My Account LogoutDocumento59 páginasMy Masterclass Exam #59765: About Products Buy Institutions Exam Demo Video Demo Contact Us FAQ My Account LogoutAhmed AbdelgelilAinda não há avaliações
- Common Cases PacesDocumento3 páginasCommon Cases PacesRohitKumarAinda não há avaliações
- GIT MnemonicsDocumento20 páginasGIT MnemonicsAhmed AbdelgelilAinda não há avaliações
- PainkillersDocumento1 páginaPainkillersAhmed AbdelgelilAinda não há avaliações
- My Masterclass Exam #58292: About Products Buy Institutions Exam Demo Video Demo Contact Us FAQ My Account LogoutDocumento59 páginasMy Masterclass Exam #58292: About Products Buy Institutions Exam Demo Video Demo Contact Us FAQ My Account LogoutAhmed AbdelgelilAinda não há avaliações
- PainkillersDocumento1 páginaPainkillersAhmed AbdelgelilAinda não há avaliações
- Doctor in Come by Service Types ReportDocumento1 páginaDoctor in Come by Service Types ReportAhmed AbdelgelilAinda não há avaliações
- Brian A .Magowan - Part 2 SbasDocumento231 páginasBrian A .Magowan - Part 2 SbasAhmed Abdelgelil75% (4)
- From: Hypertension in 2017-What Is The Right Target?Documento1 páginaFrom: Hypertension in 2017-What Is The Right Target?Ahmed AbdelgelilAinda não há avaliações
- Diagnosis and Management of Supraventricular TachycardiaDocumento9 páginasDiagnosis and Management of Supraventricular TachycardiaAhmed AbdelgelilAinda não há avaliações
- Acute Coronary Syndromes PDFDocumento13 páginasAcute Coronary Syndromes PDFAhmed AbdelgelilAinda não há avaliações
- Diagnosis and Management of Chronic Heart Failure PDFDocumento3 páginasDiagnosis and Management of Chronic Heart Failure PDFAhmed AbdelgelilAinda não há avaliações
- Self Assessment Sba .Philip BakerDocumento196 páginasSelf Assessment Sba .Philip BakerAhmed Abdelgelil100% (2)
- Self Assessment Sba .Philip BakerDocumento196 páginasSelf Assessment Sba .Philip BakerAhmed Abdelgelil100% (2)
- Content ServerDocumento13 páginasContent ServerjojdoAinda não há avaliações
- Drugs of DiabetesDocumento42 páginasDrugs of Diabeteskwennybiang100% (1)
- Pneumonia Definations & ClassificationsDocumento29 páginasPneumonia Definations & ClassificationsJimitAinda não há avaliações
- The Gravedigger's Guide To Cardiology Overview TOCDocumento58 páginasThe Gravedigger's Guide To Cardiology Overview TOCsafasayedAinda não há avaliações
- Cancer Adime NoteDocumento3 páginasCancer Adime Noteapi-436601804Ainda não há avaliações
- Introduction To Public HealthDocumento54 páginasIntroduction To Public HealthKristelle Marie Enanoria Bardon50% (2)
- Bio ReportDocumento4 páginasBio ReportKate MabanagAinda não há avaliações
- The Vaccine WatchmanDocumento46 páginasThe Vaccine WatchmanHan Gi Chase100% (2)
- Heart Attack (Myocardial Infarction) : Elevation Myocardial Infarction (STEMI) - A Partial Myocardial Infarction (NSTEMI)Documento4 páginasHeart Attack (Myocardial Infarction) : Elevation Myocardial Infarction (STEMI) - A Partial Myocardial Infarction (NSTEMI)mbok diyirAinda não há avaliações
- Nursing Care Plan For Food PoisoningDocumento1 páginaNursing Care Plan For Food Poisoningscret_gurlz9220% (5)
- CANCER Registry FormDocumento4 páginasCANCER Registry Formcar3laAinda não há avaliações
- Risk Predictors in Periodontal DiseaseDocumento8 páginasRisk Predictors in Periodontal DiseaseShreyaAinda não há avaliações
- RUHS Pre PG 2014 BDS Section II Question Paper and Answer KeyDocumento18 páginasRUHS Pre PG 2014 BDS Section II Question Paper and Answer KeyAnweshaBoseAinda não há avaliações
- Medication - ALT-Template SennaDocumento1 páginaMedication - ALT-Template SennaNancyAmissahAinda não há avaliações
- Genetic Disorders Project Rubric 17-18Documento3 páginasGenetic Disorders Project Rubric 17-18api-394564312Ainda não há avaliações
- ECG ReviewingDocumento50 páginasECG ReviewingLutfir Rahman TarisAinda não há avaliações
- Diabetes MellitusDocumento6 páginasDiabetes MellitusDr Mangesti Utami PKM Kebaman BanyuwangiAinda não há avaliações
- The Significance of SaluyotDocumento33 páginasThe Significance of SaluyotRo-Anne Nuguit - Obligar0% (1)
- Care Advantage (Health Insurance Product) Prospectus Cum Sales LiteratureDocumento42 páginasCare Advantage (Health Insurance Product) Prospectus Cum Sales Literaturevipin kumarAinda não há avaliações
- NP2 Recalls3Documento8 páginasNP2 Recalls3Larabelle Avila CoralesAinda não há avaliações
- C C W - B C - T M: U R T I (P, Urti, S, B) : (1) PharyngitisDocumento5 páginasC C W - B C - T M: U R T I (P, Urti, S, B) : (1) PharyngitiscorsaruAinda não há avaliações
- Acupuncture WordDocumento3 páginasAcupuncture WordMAC VINCEAinda não há avaliações
- Farm Safety Risk AssessmentDocumento32 páginasFarm Safety Risk AssessmentnmmartinsaAinda não há avaliações
- Work-Life Balance ResearchDocumento13 páginasWork-Life Balance ResearchHaritaa Varshini BalakumaranAinda não há avaliações
- Escaran - Drug Study - Set ADocumento4 páginasEscaran - Drug Study - Set AFrancis Alfred EscaranAinda não há avaliações
- Geriatric Nursing Terms and ConceptsDocumento53 páginasGeriatric Nursing Terms and ConceptsGodfrey FrancoAinda não há avaliações
- Original Research Article: Vitan Patel, Minal Shastri, Nisha Gaur, Prutha Jinwala, Abhishek Y. KadamDocumento5 páginasOriginal Research Article: Vitan Patel, Minal Shastri, Nisha Gaur, Prutha Jinwala, Abhishek Y. KadamTam LyAinda não há avaliações
- Wasp StingDocumento3 páginasWasp StingShruthi KyAinda não há avaliações
- Ewen Vs National Hockey LeagueDocumento80 páginasEwen Vs National Hockey LeagueAnonymous LRPtKqjQSyAinda não há avaliações
- 1.2 General Survey, Vital Signs, and SkinDocumento7 páginas1.2 General Survey, Vital Signs, and SkinC1 - RAZALAN NICKA JOYAinda não há avaliações