Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- HD 60364-7-710Documento46 páginasHD 60364-7-710LUis Faria100% (2)
- Metabolic EncephalopathyDocumento26 páginasMetabolic Encephalopathywirdahaja100% (3)
- Lesson 7Documento2 páginasLesson 7rjay manalo67% (6)
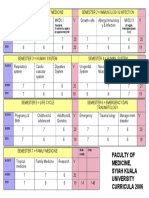
- Faculty of Medicine, Syiah Kuala University Curricula 2006Documento1 páginaFaculty of Medicine, Syiah Kuala University Curricula 2006wirdahajaAinda não há avaliações
- Microbiology - Scabies and PediculosisDocumento32 páginasMicrobiology - Scabies and PediculosiswirdahajaAinda não há avaliações
- TOEFL TEST Dan Kunci JawabanDocumento5 páginasTOEFL TEST Dan Kunci JawabanwirdahajaAinda não há avaliações
- Tinea UnguiumDocumento8 páginasTinea UnguiumwirdahajaAinda não há avaliações
- Defense Mechanism (IB)Documento60 páginasDefense Mechanism (IB)wirdahajaAinda não há avaliações
- Anatomy of The Ear HearingDocumento14 páginasAnatomy of The Ear HearingwirdahajaAinda não há avaliações
- Fever and RashDocumento14 páginasFever and RashwirdahajaAinda não há avaliações
- Clinical PathwayDocumento154 páginasClinical Pathwaywirdahaja100% (1)
- Follow Up: No Tanggal Subjektif Objektif Assessment Planning TerapiDocumento4 páginasFollow Up: No Tanggal Subjektif Objektif Assessment Planning TerapiwirdahajaAinda não há avaliações
- Medical Surgical Nursing 2nd Edition Osborn Test Bank DownloadDocumento17 páginasMedical Surgical Nursing 2nd Edition Osborn Test Bank Downloadrosakien8871yc100% (34)
- Rchl1pdf PDF CompressDocumento111 páginasRchl1pdf PDF CompressCristian CiocoiuAinda não há avaliações
- Detail Studies of Mango Qualitative Production, Its Marketing and Mango Processing Industry in Uttar PradeshDocumento156 páginasDetail Studies of Mango Qualitative Production, Its Marketing and Mango Processing Industry in Uttar PradeshPriety Verma91% (11)
- Cô Mai Phương - Đề Chuẩn 05 - File Word Có Lời Giải Chi TiếtDocumento20 páginasCô Mai Phương - Đề Chuẩn 05 - File Word Có Lời Giải Chi TiếtMinh Đức NguyễnAinda não há avaliações
- Genicular Nerve Ablation Zeitlinger2019Documento7 páginasGenicular Nerve Ablation Zeitlinger2019drjorgewtorresAinda não há avaliações
- CPC Training Centre GuidelinesDocumento28 páginasCPC Training Centre GuidelinesRight TrackAinda não há avaliações
- Comparison of 3D C-Arm Fluoroscopy and 3D Image-GuidedDocumento8 páginasComparison of 3D C-Arm Fluoroscopy and 3D Image-Guidedgevowo3277Ainda não há avaliações
- SDS Bona Cleaner UKDocumento13 páginasSDS Bona Cleaner UKObaciu Mihaela DeliaAinda não há avaliações
- Body-Weakness-Ncp X Drug StudyDocumento3 páginasBody-Weakness-Ncp X Drug Studyhayascent hilarioAinda não há avaliações
- Equipment With Moving or Rotating Parts, Use of Hazardous Hand Tools (Grinding) : The Employee's Hand Might Contact The Grinder BrushDocumento1 páginaEquipment With Moving or Rotating Parts, Use of Hazardous Hand Tools (Grinding) : The Employee's Hand Might Contact The Grinder BrushAhmedAinda não há avaliações
- PD Lesson 5 Coping With Stress in Middle and Late AdolescenceDocumento16 páginasPD Lesson 5 Coping With Stress in Middle and Late AdolescenceEL FuentesAinda não há avaliações
- Agri Fos 400 MSDSDocumento3 páginasAgri Fos 400 MSDSDaniela VargasAinda não há avaliações
- (Rev.0) E-Cube 5 - UDocumento467 páginas(Rev.0) E-Cube 5 - UMarc PolflietAinda não há avaliações
- Josseicka Reynoso ResumeDocumento1 páginaJosseicka Reynoso ResumeLouis MarchiAinda não há avaliações
- Assessment and Treatment of Spasticity: Cori Ponter, PT, MPT, NCS Barrow Neurological Institute 3/23/19Documento76 páginasAssessment and Treatment of Spasticity: Cori Ponter, PT, MPT, NCS Barrow Neurological Institute 3/23/19Praneetha100% (2)
- SiapDocumento7 páginasSiapRizky FatahAinda não há avaliações
- Test Bank For Introduction To Psychology 9th Edition PlotnikDocumento26 páginasTest Bank For Introduction To Psychology 9th Edition Plotnikheadlineuncurllfp07mAinda não há avaliações
- Quarter 4 - Module 2 Reading ComprehensionDocumento28 páginasQuarter 4 - Module 2 Reading ComprehensionMaria Kassandra Ecot50% (2)
- Bnys Manual Release Program InvitationDocumento2 páginasBnys Manual Release Program InvitationDrThangaraj KAinda não há avaliações
- Recurrent SnezzingDocumento7 páginasRecurrent Snezzingrahulsinghroy17025Ainda não há avaliações
- What's The Matter?: English Assignment Worth: 1,5Documento1 páginaWhat's The Matter?: English Assignment Worth: 1,5Teacher BrunaAinda não há avaliações
- Day 1Documento2 páginasDay 1hams byulAinda não há avaliações
- Neonatal Respiratory DistressDocumento54 páginasNeonatal Respiratory DistressMohamad Saleh100% (1)
- MINANG ES AUGUST-2022-Monthly-Instructional-Supervisory-PlanDocumento3 páginasMINANG ES AUGUST-2022-Monthly-Instructional-Supervisory-PlanPacita ImpongAinda não há avaliações
- The Different Types of InsomniaDocumento5 páginasThe Different Types of InsomniaDavid WillAinda não há avaliações
- Harm Reduction Position Paper - Final 2Documento19 páginasHarm Reduction Position Paper - Final 2G LekAinda não há avaliações
- REDCOP Updates (Reg.v)Documento36 páginasREDCOP Updates (Reg.v)DaNiel AUreusAinda não há avaliações
- Affirmations For Teenage Girls To Use Daily - DivDocumento2 páginasAffirmations For Teenage Girls To Use Daily - DivAnne CahillAinda não há avaliações