Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Tubes NclexDocumento3 páginasTubes NclexYoke W Khoo100% (1)
- Greece Dug Medicine PRICE LIST 10-1-2011 V1Documento111 páginasGreece Dug Medicine PRICE LIST 10-1-2011 V1Anuj MairhAinda não há avaliações
- A To Z Drugs-2 PDFDocumento40 páginasA To Z Drugs-2 PDFMohamedYosef71% (7)
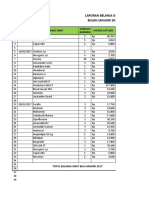
- Laporan Belanja Obat Bulan Januari 2017: No Tanggal Nama Obat Harga Satuan Jumlah BarangDocumento16 páginasLaporan Belanja Obat Bulan Januari 2017: No Tanggal Nama Obat Harga Satuan Jumlah Barangcitra husadaAinda não há avaliações
- Dapus Umum LengkapDocumento6 páginasDapus Umum LengkapDhewiantyAinda não há avaliações
- 2017 (Laporan Pelayanan Rawat Jalan Dr. Ida Ayu Anom Margareni)Documento11 páginas2017 (Laporan Pelayanan Rawat Jalan Dr. Ida Ayu Anom Margareni)Anggi RiyaniAinda não há avaliações
- Rusan Pharma Product ListDocumento4 páginasRusan Pharma Product ListSanjay SharmaAinda não há avaliações
- Catalogo Petmedical Nov22Documento14 páginasCatalogo Petmedical Nov22Emile CardAinda não há avaliações
- Progress Note ExampleDocumento1 páginaProgress Note ExampleMohamed HushainAinda não há avaliações
- CRT Exam Review Guide Chapter 16Documento16 páginasCRT Exam Review Guide Chapter 16Dharlyn MungcalAinda não há avaliações
- HOSPITAL Past PapersDocumento6 páginasHOSPITAL Past PapersMr nobodyAinda não há avaliações
- UPT Puskesmas Cijagra Lama: Pengurus Barang Pembantu Bandung, 31 Maret 2018Documento6 páginasUPT Puskesmas Cijagra Lama: Pengurus Barang Pembantu Bandung, 31 Maret 2018Mutty Arra Zya RiezthicaAinda não há avaliações
- Off Exclusivity DrugsDocumento17 páginasOff Exclusivity DrugsJagdish ChanderAinda não há avaliações
- Asthma 017Documento46 páginasAsthma 017Mariam AlavidzeAinda não há avaliações
- Mengklasifikasi Perbekalan FarmasiDocumento56 páginasMengklasifikasi Perbekalan FarmasiAenhiequrra AlthafunnisaAinda não há avaliações
- Vademecum Ips SaltaDocumento141 páginasVademecum Ips SaltaGabriela Fernanda LopezAinda não há avaliações
- Ecart DrugsDocumento1 páginaEcart DrugsKarla JaneAinda não há avaliações
- Pcac - Ucm486146Documento429 páginasPcac - Ucm486146leoncioAinda não há avaliações
- Drug Education Definition of Terms: Acute ToleranceDocumento6 páginasDrug Education Definition of Terms: Acute ToleranceAldrin CrutoAinda não há avaliações
- MIDAZOLAM Drug StudyDocumento3 páginasMIDAZOLAM Drug StudyEur Miole60% (5)
- PHA NotesDocumento12 páginasPHA NotesMag LigAinda não há avaliações
- Immunosuppressive DrugsDocumento16 páginasImmunosuppressive DrugsU2103586 STUDENTAinda não há avaliações
- Standard Medication Administration TimesDocumento4 páginasStandard Medication Administration TimesMark Anthony C. SerilAinda não há avaliações
- Pharma Drug SufficesDocumento3 páginasPharma Drug SufficesJillian GayleAinda não há avaliações
- Spinal AnesthesiaDocumento5 páginasSpinal Anesthesiaakif48266Ainda não há avaliações
- Drug Card GardasilDocumento2 páginasDrug Card GardasilJuliaAinda não há avaliações
- List Obat High AlertDocumento5 páginasList Obat High AlertCHRISTINE EriskaAinda não há avaliações
- Reference Guide For Pharmacy Technician Exam: Manan ShroffDocumento50 páginasReference Guide For Pharmacy Technician Exam: Manan ShroffAira Gene Meneses100% (2)
- 2020 Conference PaperDocumento2 páginas2020 Conference PaperHealthcare Pro LearningAinda não há avaliações
- MetabolicsyndDocumento37 páginasMetabolicsyndShanooha MansoorAinda não há avaliações