Você também pode gostar
- Optic Nerve (CN II) Anatomy and PhysiologyDocumento12 páginasOptic Nerve (CN II) Anatomy and PhysiologyWahab RasyidAinda não há avaliações
- Optic Nerve: Presented By: Aqsa Irfan Presented To: Dr. Sania ZehraDocumento21 páginasOptic Nerve: Presented By: Aqsa Irfan Presented To: Dr. Sania ZehraAqsaAinda não há avaliações
- Swings light from one eye to otherPatient: Pupil constricts only when light is shone on eye and not when light is shone on other eyeIndicates relative afferent pupillary defect (RAPDDocumento39 páginasSwings light from one eye to otherPatient: Pupil constricts only when light is shone on eye and not when light is shone on other eyeIndicates relative afferent pupillary defect (RAPDAdarsh KeshariAinda não há avaliações
- Oculomotor Nerve: DR / Hytham NafadyDocumento52 páginasOculomotor Nerve: DR / Hytham NafadyGetLyricsAinda não há avaliações
- Oculomotor Nerve 3Documento30 páginasOculomotor Nerve 3Sanreet RandhawaAinda não há avaliações
- Visual PathwayDocumento24 páginasVisual PathwayAkshara Eye FoundationAinda não há avaliações
- ANATOMY OF THE EYE (Organ of Vision) by DR Omeje EmmanuelDocumento31 páginasANATOMY OF THE EYE (Organ of Vision) by DR Omeje Emmanuelchidera100% (1)
- Optic NerveDocumento71 páginasOptic Nervelakshmi bhavanaAinda não há avaliações
- The Pupillary Light Reflex PathwayDocumento5 páginasThe Pupillary Light Reflex PathwayNauli PanjaitanAinda não há avaliações
- The Swinging Flashlight Test: Learning Objective: Facts About The PupilDocumento3 páginasThe Swinging Flashlight Test: Learning Objective: Facts About The Pupilsiti hazard aldinaAinda não há avaliações
- Cranial Nerve Nadz FinalDocumento58 páginasCranial Nerve Nadz Finalnadzirah ruslanAinda não há avaliações
- Pupillary Dilatation ReflexDocumento7 páginasPupillary Dilatation ReflexEden Canonizado ChengAinda não há avaliações
- Visual Pathway Anatomy and Pupillary Reflex AbnormalitiesDocumento43 páginasVisual Pathway Anatomy and Pupillary Reflex AbnormalitiesAdarsh KeshariAinda não há avaliações
- Pupillary Pathways &reactions: Assistant Professor, Department of Ophthalmology Nepalgunj Medical CollegeDocumento16 páginasPupillary Pathways &reactions: Assistant Professor, Department of Ophthalmology Nepalgunj Medical CollegeDrBikram ThapaAinda não há avaliações
- AdelineDocumento34 páginasAdelineEmmanuel NdukaAinda não há avaliações
- Vertebral Arteries, and Their Divisions. Arteries Fuse To Form The Basilar ArteryDocumento6 páginasVertebral Arteries, and Their Divisions. Arteries Fuse To Form The Basilar Arterymurali_bharadwazAinda não há avaliações
- Development of EyeDocumento21 páginasDevelopment of Eyeklauss starAinda não há avaliações
- Blood Suppy of BrainDocumento54 páginasBlood Suppy of BrainZoya MoraniAinda não há avaliações
- Histology of Kidney, Ureter and BladderDocumento28 páginasHistology of Kidney, Ureter and Bladderkhairul_azhar_27Ainda não há avaliações
- TF00001028 (Autosaved)Documento10 páginasTF00001028 (Autosaved)Cid MusaAinda não há avaliações
- Post Y-Shunt Brain Abscess Case ReportDocumento2 páginasPost Y-Shunt Brain Abscess Case ReportArif PebriantoAinda não há avaliações
- The Ventricular SystemDocumento6 páginasThe Ventricular SystemM Arsalan TariqAinda não há avaliações
- Anterior Triangle of The Neck IIDocumento49 páginasAnterior Triangle of The Neck IIvrajAinda não há avaliações
- Motor TractDocumento4 páginasMotor TractRaden Achmad Candra PutraAinda não há avaliações
- Venous Blood Sinuses Guide: Anatomy, Drainage & Clinical NotesDocumento15 páginasVenous Blood Sinuses Guide: Anatomy, Drainage & Clinical NotesJennifer RodriguezAinda não há avaliações
- Visual Field Defect Case ReportDocumento25 páginasVisual Field Defect Case Report033010969Ainda não há avaliações
- Complete Neurologic ExamDocumento21 páginasComplete Neurologic ExamRaymond CruzAinda não há avaliações
- Posterior Triangle of Neck Anatomy and Clinical ApplicationsDocumento34 páginasPosterior Triangle of Neck Anatomy and Clinical ApplicationssnehalkmAinda não há avaliações
- Pupillary Pathway Explained: Nerves, Reflexes and ExaminationDocumento21 páginasPupillary Pathway Explained: Nerves, Reflexes and ExaminationSurbhi BhartiAinda não há avaliações
- Blood Supply of The BrainDocumento11 páginasBlood Supply of The Brainneleh grayAinda não há avaliações
- Visual Pathway & Its LesionsDocumento24 páginasVisual Pathway & Its LesionsSyedaNaveenBatoolAinda não há avaliações
- Clinical Approach To Brainstem LesionsDocumento10 páginasClinical Approach To Brainstem LesionsJosé SánchezAinda não há avaliações
- Pupillary Reflexes: Rohith. A Roll No-66Documento34 páginasPupillary Reflexes: Rohith. A Roll No-66KarthikeyanAinda não há avaliações
- Blood Supply of The BrainDocumento55 páginasBlood Supply of The BrainueumanaAinda não há avaliações
- ORBITDocumento46 páginasORBITdr yati gothwalAinda não há avaliações
- Classification of Nerve Fibers: Types and FunctionsDocumento21 páginasClassification of Nerve Fibers: Types and FunctionsNayab IftikharAinda não há avaliações
- Examining Histologic SlidesDocumento104 páginasExamining Histologic SlidesVlad TomaAinda não há avaliações
- Blood Supply of BrainDocumento49 páginasBlood Supply of BrainDarling Sevenfoldism SynysterAinda não há avaliações
- Somatosensory Pathways: Primary Sensory and Motor AreasDocumento36 páginasSomatosensory Pathways: Primary Sensory and Motor AreasAnonymous w3vYureAinda não há avaliações
- Neuro-Ophthalmology: DR Jusuf Wijaya, SPM FK - Uki CawangDocumento65 páginasNeuro-Ophthalmology: DR Jusuf Wijaya, SPM FK - Uki CawanggeorgyAinda não há avaliações
- 734 Visual Pathway LesionsDocumento25 páginas734 Visual Pathway LesionsNarendra N NaruAinda não há avaliações
- Sectional Anatomy of the Brain: Understanding Brain Structures in 2D and 3DDocumento30 páginasSectional Anatomy of the Brain: Understanding Brain Structures in 2D and 3DLazaros TsiatsiosAinda não há avaliações
- Cranial Neuropathies Guide: Electrodiagnosis and ManagementDocumento74 páginasCranial Neuropathies Guide: Electrodiagnosis and ManagementKevin Woodard100% (1)
- Cerebellum and Brain Stem: DR Asim Shrestha SRCC Ped Neuro Fellow MumbaiDocumento71 páginasCerebellum and Brain Stem: DR Asim Shrestha SRCC Ped Neuro Fellow MumbaiAsim ShresthaAinda não há avaliações
- 24 Cerebral Blood FlowDocumento31 páginas24 Cerebral Blood FlowZuhaib Ahmed100% (1)
- Head and Spinal Cord Injury (Ci)Documento111 páginasHead and Spinal Cord Injury (Ci)azmerawAinda não há avaliações
- Peripheral Nerve Injury and Repair: Adam Osbourne, 5th Year MedicineDocumento5 páginasPeripheral Nerve Injury and Repair: Adam Osbourne, 5th Year Medicineayrahma29Ainda não há avaliações
- Nerve TractsDocumento38 páginasNerve TractsAbualauon AlbeblawyAinda não há avaliações
- Anatomy Pupillary Pathways AND Abnormal Pupils: Dr. Ravula Hasika M.S.Ophthalmology (1 YR)Documento100 páginasAnatomy Pupillary Pathways AND Abnormal Pupils: Dr. Ravula Hasika M.S.Ophthalmology (1 YR)Sonia Afika AzizaAinda não há avaliações
- Oculomotor Nerve: Arista Prima NDocumento7 páginasOculomotor Nerve: Arista Prima NArista Prima N100% (1)
- Anatomy of Labyrinth by DR Inam Ur RehmanDocumento29 páginasAnatomy of Labyrinth by DR Inam Ur RehmanasssadulllahAinda não há avaliações
- Neuro 3 Brainstem and Spinal Cord BriefDocumento68 páginasNeuro 3 Brainstem and Spinal Cord BriefYasimini Ramadhani100% (1)
- PONS: NeuroanatomyDocumento20 páginasPONS: NeuroanatomyHassan IlyasAinda não há avaliações
- Rehabilitation Handbook for Stroke CliniciansDocumento29 páginasRehabilitation Handbook for Stroke CliniciansDedi SutiaAinda não há avaliações
- Traktus UveaDocumento90 páginasTraktus UveaAudrey Ira Yunita100% (1)
- Anatomy of Cerebral Blood Supply & Cerebral PhysiologyDocumento32 páginasAnatomy of Cerebral Blood Supply & Cerebral Physiologykiran kizhakkiniAinda não há avaliações
- Physiology of Hearing and Equilibrium LectureDocumento52 páginasPhysiology of Hearing and Equilibrium LectureHomeground entertainment100% (1)
- 13 Subjective RefractionDocumento19 páginas13 Subjective Refractionmuhammad farizAinda não há avaliações
- ANATOMY AND PHYSIOLOGY OF THE OPTIC NERVEDocumento61 páginasANATOMY AND PHYSIOLOGY OF THE OPTIC NERVENaman MishraAinda não há avaliações
- Guidelines For Strengthening A&E Services in Hospitals Corrected VersionDocumento33 páginasGuidelines For Strengthening A&E Services in Hospitals Corrected VersionMohamed IrshaAinda não há avaliações
- Transfer Summary Form Hha To Hospital PDFDocumento2 páginasTransfer Summary Form Hha To Hospital PDFsafasayedAinda não há avaliações
- Ed Trauma Flow Sheet: Part of The Medical RecordDocumento6 páginasEd Trauma Flow Sheet: Part of The Medical RecordsafasayedAinda não há avaliações
- HistoryandPhysicalExamDocumento105 páginasHistoryandPhysicalExamsilentscream0618Ainda não há avaliações
- S17820en PDFDocumento433 páginasS17820en PDFsafasayedAinda não há avaliações
- Dovercourt Surgery: 3 Skye Edge Avenue Sheffield S2 5FXDocumento4 páginasDovercourt Surgery: 3 Skye Edge Avenue Sheffield S2 5FXsafasayedAinda não há avaliações
- The Gravedigger's Guide To Cardiology Overview TOCDocumento58 páginasThe Gravedigger's Guide To Cardiology Overview TOCsafasayedAinda não há avaliações
- Levels 4–6 Hospitals Clinical GuidelinesDocumento574 páginasLevels 4–6 Hospitals Clinical GuidelinesavicennaxAinda não há avaliações
- Policy of E.DDocumento68 páginasPolicy of E.DsafasayedAinda não há avaliações
- Adult Health Status Summary: Page 1 of 3Documento3 páginasAdult Health Status Summary: Page 1 of 3safasayedAinda não há avaliações
- NICUDocumento190 páginasNICUsafasayedAinda não há avaliações
- ACLS Adult Cardiac Arrest AlgorithmDocumento1 páginaACLS Adult Cardiac Arrest AlgorithmTasya ShafiraAinda não há avaliações
- Guidelines For Intensive Care Unit DesignDocumento15 páginasGuidelines For Intensive Care Unit DesignDiego Fernando OvalleAinda não há avaliações
- King's College Hospital Early Pregnancy Unit Referral: Mon - Fri, 9am - 12pmDocumento1 páginaKing's College Hospital Early Pregnancy Unit Referral: Mon - Fri, 9am - 12pmsafasayedAinda não há avaliações
- Family MedicineDocumento194 páginasFamily Medicineapi-3712326100% (2)
- Malaria 2Documento1 páginaMalaria 2jvAinda não há avaliações
- 01 Training in IrelandDocumento17 páginas01 Training in IrelandsafasayedAinda não há avaliações
- ESCRS EndophthalmitisDocumento52 páginasESCRS EndophthalmitisKaveh Vahdani100% (2)
- HistoryandPhysicalExamDocumento105 páginasHistoryandPhysicalExamsilentscream0618Ainda não há avaliações
- Daily Repositioning Skin Inspection ChartDocumento2 páginasDaily Repositioning Skin Inspection Chartsafasayed100% (1)
- Malaria 2Documento1 páginaMalaria 2jvAinda não há avaliações
- Sri Lakshmi Medical Centre and Hospital: 18/121 MTP Road, Thudiyalur, Coimbatore - 641 034Documento49 páginasSri Lakshmi Medical Centre and Hospital: 18/121 MTP Road, Thudiyalur, Coimbatore - 641 034dhir.ankur100% (1)
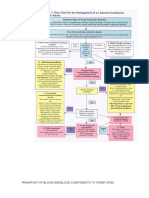
- Transport of Blood and Blood Components To Other SitesDocumento8 páginasTransport of Blood and Blood Components To Other SitessafasayedAinda não há avaliações
- Transfer Summary Form Hha To Hospital PDFDocumento2 páginasTransfer Summary Form Hha To Hospital PDFsafasayedAinda não há avaliações
- JP Medical Doctor MSF For Alexandria 052015 PDFDocumento2 páginasJP Medical Doctor MSF For Alexandria 052015 PDFsafasayedAinda não há avaliações
- Improving Admission and Discharge PerformanceDocumento11 páginasImproving Admission and Discharge PerformancesafasayedAinda não há avaliações
- 01 Training in IrelandDocumento17 páginas01 Training in IrelandsafasayedAinda não há avaliações
- WATO EX-35 Anesthesia Machine Order InformationDocumento4 páginasWATO EX-35 Anesthesia Machine Order InformationsafasayedAinda não há avaliações
- BasalBolusProtocol InsulinDocumento2 páginasBasalBolusProtocol InsulinsafasayedAinda não há avaliações
- ZONCARE-Q7 (95) Product Introduction - LilyDocumento48 páginasZONCARE-Q7 (95) Product Introduction - LilysafasayedAinda não há avaliações
- Component 2 Learner Statement Y2Documento6 páginasComponent 2 Learner Statement Y2api-426152133Ainda não há avaliações
- Money MBA 1Documento4 páginasMoney MBA 1neaman_ahmed0% (1)
- Balzac and the Little Chinese Seamstress: A Journey During the Cultural RevolutionDocumento4 páginasBalzac and the Little Chinese Seamstress: A Journey During the Cultural RevolutionRogona 123Ainda não há avaliações
- Lorain Schools CEO Finalist Lloyd MartinDocumento14 páginasLorain Schools CEO Finalist Lloyd MartinThe Morning JournalAinda não há avaliações
- WP1019 CharterDocumento5 páginasWP1019 CharternocnexAinda não há avaliações
- Manufacturing Tech-1Documento6 páginasManufacturing Tech-1Vikram Rao0% (1)
- Accounting Students' Attitude Towads AccountingDocumento29 páginasAccounting Students' Attitude Towads AccountingSham Salonga Pascual50% (2)
- EA Flora 1Documento3 páginasEA Flora 1A. MagnoAinda não há avaliações
- Pub - Perspectives On Global Cultures Issues in Cultural PDFDocumento190 páginasPub - Perspectives On Global Cultures Issues in Cultural PDFCherlyn Jane Ventura TuliaoAinda não há avaliações
- PMMC ExperimentDocumento2 páginasPMMC ExperimentShyam ShankarAinda não há avaliações
- Product Differentiation and Market Segmentation As Alternative Marketing StrategiesDocumento7 páginasProduct Differentiation and Market Segmentation As Alternative Marketing StrategiesCaertiMAinda não há avaliações
- Explore Spanish Lesson Plan - AnimalsDocumento8 páginasExplore Spanish Lesson Plan - Animalsapi-257582917Ainda não há avaliações
- DionWIred Black FridayDocumento13 páginasDionWIred Black FridayAmon SimelaneAinda não há avaliações
- Linear Piston Actuators: by Sekhar Samy, CCI, and Dave Stemler, CCIDocumento18 páginasLinear Piston Actuators: by Sekhar Samy, CCI, and Dave Stemler, CCIapi-3854910Ainda não há avaliações
- Laboratory SafetyDocumento4 páginasLaboratory SafetyLey DoydoraAinda não há avaliações
- Thank you for purchasing your remap from HDI Tuning LtdDocumento2 páginasThank you for purchasing your remap from HDI Tuning LtdMaks LebanAinda não há avaliações
- Anki Very Useful ManualDocumento5 páginasAnki Very Useful ManualSoundaryaAinda não há avaliações
- Osprey, Men-At-Arms #008 The Black Watch (1971) (-) OCR 8.12Documento48 páginasOsprey, Men-At-Arms #008 The Black Watch (1971) (-) OCR 8.12mancini100% (4)
- Intro - S4HANA - Using - Global - Bike - Slides - MM - en - v3.3 MODDocumento45 páginasIntro - S4HANA - Using - Global - Bike - Slides - MM - en - v3.3 MODMrThedjalexAinda não há avaliações
- Adjutant-Introuvable BASIC VERSIONDocumento7 páginasAdjutant-Introuvable BASIC VERSIONfurrypdfAinda não há avaliações
- Predictive Analytics: QM901.1x Prof U Dinesh Kumar, IIMBDocumento36 páginasPredictive Analytics: QM901.1x Prof U Dinesh Kumar, IIMBVenkata Nelluri PmpAinda não há avaliações
- SID-2AF User Manual English V3.04Documento39 páginasSID-2AF User Manual English V3.04om_zahidAinda não há avaliações
- FAI - Assignment Sheet (Both Assignments)Documento5 páginasFAI - Assignment Sheet (Both Assignments)Wilson WongAinda não há avaliações
- Unit Test Nervous System 14.1Documento4 páginasUnit Test Nervous System 14.1ArnelAinda não há avaliações
- Anticipate Problems Before They Emerge: White PaperDocumento7 páginasAnticipate Problems Before They Emerge: White PaperYotsapol KantaratAinda não há avaliações
- Resp Part 4Documento95 páginasResp Part 4Kristian CadaAinda não há avaliações
- Why Leaders Should Look in the “MirrorDocumento4 páginasWhy Leaders Should Look in the “MirrorCaryl Baylon EstreraAinda não há avaliações
- CH 21Documento70 páginasCH 21Shakib Ahmed Emon 0389Ainda não há avaliações
- Transistor Amplifier Operating ParametersDocumento21 páginasTransistor Amplifier Operating ParametersReddyvari VenugopalAinda não há avaliações
- Biology GCE 2010 June Paper 1 Mark SchemeDocumento10 páginasBiology GCE 2010 June Paper 1 Mark SchemeRicky MartinAinda não há avaliações