Você também pode gostar
- EmbryologyDocumento28 páginasEmbryologyKamleshwari RenganathanAinda não há avaliações
- Anatomy Pupillary Pathways AND Abnormal Pupils: Dr. Ravula Hasika M.S.Ophthalmology (1 YR)Documento100 páginasAnatomy Pupillary Pathways AND Abnormal Pupils: Dr. Ravula Hasika M.S.Ophthalmology (1 YR)Sonia Afika Aziza100% (1)
- Development of EyeDocumento21 páginasDevelopment of Eyeklauss starAinda não há avaliações
- Anatomy and Physiology of The EyesDocumento3 páginasAnatomy and Physiology of The EyesNkk Aqnd MgdnglAinda não há avaliações
- Pupillary Pathway, Pupillary Abnormalities, RAPDDocumento24 páginasPupillary Pathway, Pupillary Abnormalities, RAPD015Afeefa N AAinda não há avaliações
- Anatomy and Physiology of Optic Nerve.: Dr. Sumit Pandey, MD Lecturer, COMSDocumento61 páginasAnatomy and Physiology of Optic Nerve.: Dr. Sumit Pandey, MD Lecturer, COMSNaman Mishra100% (1)
- ANATOMY OF THE EYE (Organ of Vision) by DR Omeje EmmanuelDocumento31 páginasANATOMY OF THE EYE (Organ of Vision) by DR Omeje Emmanuelchidera100% (2)
- AnaPhy Lab FinalDocumento7 páginasAnaPhy Lab FinalGian RafananAinda não há avaliações
- Pupillary PathwayDocumento21 páginasPupillary PathwaySurbhi BhartiAinda não há avaliações
- Optic Nerve (Cranial Nerve Ii) : Abdul Wahab RasyidDocumento12 páginasOptic Nerve (Cranial Nerve Ii) : Abdul Wahab RasyidWahab Rasyid100% (1)
- The OrbitDocumento115 páginasThe OrbitPhilip McNelson100% (1)
- Pupillary Dilatation ReflexDocumento7 páginasPupillary Dilatation ReflexEden Canonizado ChengAinda não há avaliações
- EyeDocumento50 páginasEyedavid100% (1)
- NED Proposal & Budget GuidelinesDocumento10 páginasNED Proposal & Budget Guidelinesayeaye2015Ainda não há avaliações
- The Swinging Flashlight Test: Learning Objective: Facts About The PupilDocumento3 páginasThe Swinging Flashlight Test: Learning Objective: Facts About The Pupilsiti hazard aldinaAinda não há avaliações
- Pupillary Pathways &reactions: Assistant Professor, Department of Ophthalmology Nepalgunj Medical CollegeDocumento16 páginasPupillary Pathways &reactions: Assistant Professor, Department of Ophthalmology Nepalgunj Medical CollegeDrBikram ThapaAinda não há avaliações
- Anatomy and Physiology of Visual PathwayDocumento39 páginasAnatomy and Physiology of Visual PathwayAdarsh KeshariAinda não há avaliações
- Visual ND Pupillary PathwayDocumento43 páginasVisual ND Pupillary PathwayAdarsh KeshariAinda não há avaliações
- The Pupillary Light Reflex PathwayDocumento5 páginasThe Pupillary Light Reflex PathwayNauli PanjaitanAinda não há avaliações
- Optic Nerve: Presented By: Aqsa Irfan Presented To: Dr. Sania ZehraDocumento21 páginasOptic Nerve: Presented By: Aqsa Irfan Presented To: Dr. Sania ZehraAqsaAinda não há avaliações
- Common Eye Diseases 2022Documento33 páginasCommon Eye Diseases 2022Shia LevyAinda não há avaliações
- Optic NerveDocumento71 páginasOptic Nervelakshmi bhavana100% (1)
- Complete Neurologic ExamDocumento21 páginasComplete Neurologic ExamRaymond CruzAinda não há avaliações
- Ophthalmology V Eye Anatomy and FunctionDocumento45 páginasOphthalmology V Eye Anatomy and FunctionEndale AschenakiAinda não há avaliações
- Anatomy of Visual Pathway, Field Defects AND Its Lesions.: By-Dr. Ruchi PherwaniDocumento43 páginasAnatomy of Visual Pathway, Field Defects AND Its Lesions.: By-Dr. Ruchi Pherwanisafasayed100% (1)
- Cranial Nerve Nadz FinalDocumento58 páginasCranial Nerve Nadz Finalnadzirah ruslanAinda não há avaliações
- Cranial Nerve Examination OSCE GuideDocumento26 páginasCranial Nerve Examination OSCE GuideAbdullah Basheer AL-AnaziAinda não há avaliações
- The Concept Paper: Automatic ZoomDocumento4 páginasThe Concept Paper: Automatic Zoomchelsea kayle licomes fuentesAinda não há avaliações
- Pathways For Light Near ReflexesDocumento30 páginasPathways For Light Near ReflexesMalik Allahbachaya100% (1)
- Oculomotor Nerve: DR / Hytham NafadyDocumento52 páginasOculomotor Nerve: DR / Hytham NafadyGetLyricsAinda não há avaliações
- Pupiliary PathwayDocumento91 páginasPupiliary Pathwaydrsrp8467% (3)
- Anatomy of Eyelid: Presenter:-Dr. Vijayalaxmi Moderator:-Dr. SanjanaDocumento49 páginasAnatomy of Eyelid: Presenter:-Dr. Vijayalaxmi Moderator:-Dr. SanjanaRidhi Bhandari100% (1)
- Pupil Respose AssessmentDocumento4 páginasPupil Respose AssessmentRrichard Prieto MmallariAinda não há avaliações
- Embryology of Eye - 1Documento12 páginasEmbryology of Eye - 1Maitha AlwhshiAinda não há avaliações
- Cranial NervesDocumento29 páginasCranial NervesMadalina DutanAinda não há avaliações
- Oculomotor Nerve: Arista Prima NDocumento7 páginasOculomotor Nerve: Arista Prima NArista Prima N100% (1)
- Blood Supply, Nerve Supply and Lymphatics of The OrbitDocumento28 páginasBlood Supply, Nerve Supply and Lymphatics of The OrbitPallavi Uday NaikAinda não há avaliações
- Organs of VisionDocumento3 páginasOrgans of VisionNarasimha Murthy100% (1)
- Color Vision PDFDocumento59 páginasColor Vision PDFDhrubo Adhikary100% (1)
- Anatomy of RetinaDocumento39 páginasAnatomy of Retinadr_dev100% (1)
- Visual Pathway & Its LesionsDocumento24 páginasVisual Pathway & Its LesionsSyedaNaveenBatoolAinda não há avaliações
- Guidelines For The Submission of Funding RequestsDocumento12 páginasGuidelines For The Submission of Funding RequestsjnakakandeAinda não há avaliações
- Week 4 - Development of The EyeDocumento5 páginasWeek 4 - Development of The EyeAleia GoAinda não há avaliações
- Oculomotor Nerve 3Documento30 páginasOculomotor Nerve 3Sanreet RandhawaAinda não há avaliações
- Embryology of EyeDocumento28 páginasEmbryology of Eyesamuelpnrj25100% (2)
- Eye, Orbit, Orbital Region, andDocumento72 páginasEye, Orbit, Orbital Region, andSmartyna Sophia100% (1)
- Eye AssessmentDocumento7 páginasEye AssessmentPuviyarasiAinda não há avaliações
- Eye Care IntroductionDocumento66 páginasEye Care IntroductionEdeti RoneAinda não há avaliações
- Physiology of Eye. Physiology of VisionDocumento27 páginasPhysiology of Eye. Physiology of VisionSmartcool So100% (1)
- Visual SystemDocumento37 páginasVisual SystemmalindaAinda não há avaliações
- Disorders of Lashes: 1. Trichiasis 2. Metaplastic Lashes 3. Distichiasis 4. Phthiriasis Palpebrarum 5. MadarosisDocumento8 páginasDisorders of Lashes: 1. Trichiasis 2. Metaplastic Lashes 3. Distichiasis 4. Phthiriasis Palpebrarum 5. MadarosisAhmed YounisAinda não há avaliações
- Eyelids Eyelids: 7 Semester Dr. Monika Mahat 3 Year Resident Ophthalmology Department LMCTHDocumento64 páginasEyelids Eyelids: 7 Semester Dr. Monika Mahat 3 Year Resident Ophthalmology Department LMCTHSubash BasnetAinda não há avaliações
- Medical Neuroscience Tutorial Notes: Blood Supply To The BrainDocumento6 páginasMedical Neuroscience Tutorial Notes: Blood Supply To The BrainsoyyosoloyoAinda não há avaliações
- Ocular AnatomyDocumento39 páginasOcular AnatomyShilvi ShahAinda não há avaliações
- Pupillary Reflexes: Rohith. A Roll No-66Documento34 páginasPupillary Reflexes: Rohith. A Roll No-66KarthikeyanAinda não há avaliações
- Histology of Kidney, Ureter and Urinary BladderDocumento28 páginasHistology of Kidney, Ureter and Urinary Bladderkhairul_azhar_27Ainda não há avaliações
- Optic NeuritisDocumento32 páginasOptic NeuritisNajaf Ali Khan100% (1)
- Ocular EmergenciesDocumento4 páginasOcular EmergenciesJim Jose AntonyAinda não há avaliações
- Anatomy of Optic Disc and Congenital AnomalyDocumento49 páginasAnatomy of Optic Disc and Congenital AnomalyAdarsh KeshariAinda não há avaliações
- Low Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsNo EverandLow Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsAinda não há avaliações
- S17820en PDFDocumento433 páginasS17820en PDFsafasayedAinda não há avaliações
- Ed Trauma Flow Sheet: Part of The Medical RecordDocumento6 páginasEd Trauma Flow Sheet: Part of The Medical RecordsafasayedAinda não há avaliações
- The Gravedigger's Guide To Cardiology Overview TOCDocumento58 páginasThe Gravedigger's Guide To Cardiology Overview TOCsafasayedAinda não há avaliações
- Guidelines For Strengthening A&E Services in Hospitals Corrected VersionDocumento33 páginasGuidelines For Strengthening A&E Services in Hospitals Corrected VersionMohamed IrshaAinda não há avaliações
- Dovercourt Surgery: 3 Skye Edge Avenue Sheffield S2 5FXDocumento4 páginasDovercourt Surgery: 3 Skye Edge Avenue Sheffield S2 5FXsafasayedAinda não há avaliações
- Transfer Summary Form Hha To Hospital PDFDocumento2 páginasTransfer Summary Form Hha To Hospital PDFsafasayedAinda não há avaliações
- ACLS Adult Cardiac Arrest AlgorithmDocumento1 páginaACLS Adult Cardiac Arrest AlgorithmTasya ShafiraAinda não há avaliações
- HistoryandPhysicalExamDocumento105 páginasHistoryandPhysicalExamsilentscream0618Ainda não há avaliações
- S21000en PDFDocumento574 páginasS21000en PDFavicennaxAinda não há avaliações
- Guidelines For Intensive Care Unit DesignDocumento15 páginasGuidelines For Intensive Care Unit DesignDiego Fernando OvalleAinda não há avaliações
- NICUDocumento190 páginasNICUsafasayedAinda não há avaliações
- 01 Training in IrelandDocumento17 páginas01 Training in IrelandsafasayedAinda não há avaliações
- King's College Hospital Early Pregnancy Unit Referral: Mon - Fri, 9am - 12pmDocumento1 páginaKing's College Hospital Early Pregnancy Unit Referral: Mon - Fri, 9am - 12pmsafasayedAinda não há avaliações
- Adult Health Status Summary: Page 1 of 3Documento3 páginasAdult Health Status Summary: Page 1 of 3safasayedAinda não há avaliações
- Sri Lakshmi Medical Centre and Hospital: 18/121 MTP Road, Thudiyalur, Coimbatore - 641 034Documento49 páginasSri Lakshmi Medical Centre and Hospital: 18/121 MTP Road, Thudiyalur, Coimbatore - 641 034dhir.ankur100% (1)
- Family MedicineDocumento194 páginasFamily Medicineapi-3712326100% (2)
- Policy of E.DDocumento68 páginasPolicy of E.DsafasayedAinda não há avaliações
- Daily Repositioning Skin Inspection ChartDocumento2 páginasDaily Repositioning Skin Inspection Chartsafasayed100% (1)
- HistoryandPhysicalExamDocumento105 páginasHistoryandPhysicalExamsilentscream0618Ainda não há avaliações
- Transfer Summary Form Hha To Hospital PDFDocumento2 páginasTransfer Summary Form Hha To Hospital PDFsafasayedAinda não há avaliações
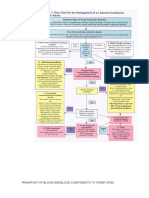
- Transport of Blood and Blood Components To Other SitesDocumento8 páginasTransport of Blood and Blood Components To Other SitessafasayedAinda não há avaliações
- BasalBolusProtocol InsulinDocumento2 páginasBasalBolusProtocol InsulinsafasayedAinda não há avaliações
- G Item 7.4A - Admission and Discharge PolicyDocumento11 páginasG Item 7.4A - Admission and Discharge PolicysafasayedAinda não há avaliações
- Malaria 2Documento1 páginaMalaria 2jvAinda não há avaliações
- JP Medical Doctor MSF For Alexandria 052015 PDFDocumento2 páginasJP Medical Doctor MSF For Alexandria 052015 PDFsafasayedAinda não há avaliações
- ESCRS EndophthalmitisDocumento52 páginasESCRS EndophthalmitisKaveh Vahdani100% (2)
- ZONCARE-Q7 (95) Product Introduction - LilyDocumento48 páginasZONCARE-Q7 (95) Product Introduction - LilysafasayedAinda não há avaliações
- Malaria 2Documento1 páginaMalaria 2jvAinda não há avaliações
- 01 Training in IrelandDocumento17 páginas01 Training in IrelandsafasayedAinda não há avaliações
- 03 Brochure WATO-EX 35Documento4 páginas03 Brochure WATO-EX 35safasayedAinda não há avaliações
- Child Protection Training ManualDocumento229 páginasChild Protection Training Manualbabuin1Ainda não há avaliações
- Circulatory Disease ProjectDocumento2 páginasCirculatory Disease Projectapi-517831630Ainda não há avaliações
- Abdominal Health AssessmentDocumento11 páginasAbdominal Health Assessmentcrisel costalesAinda não há avaliações
- Formative Gen EdDocumento119 páginasFormative Gen EdDan GertezAinda não há avaliações
- CP 01708016Documento11 páginasCP 01708016telur_kudaAinda não há avaliações
- Anatomy and Physiology of Male Reproductive SystemDocumento8 páginasAnatomy and Physiology of Male Reproductive SystemAdor AbuanAinda não há avaliações
- 4UFZ75PF0FYRH8 4UFZ75PF0FYRH8 : Division of Forensic SciencesDocumento7 páginas4UFZ75PF0FYRH8 4UFZ75PF0FYRH8 : Division of Forensic SciencesAttila KissAinda não há avaliações
- Cerebrospinal FluidDocumento12 páginasCerebrospinal FluidPavithran PAinda não há avaliações
- IELTS Recent Actual Test With Answers Practice Test 30Documento14 páginasIELTS Recent Actual Test With Answers Practice Test 30Ferris Wheel GuyAinda não há avaliações
- Common Mistakes-BiologyDocumento8 páginasCommon Mistakes-BiologyteahockAinda não há avaliações
- Imaging of Kidney Cancer - GuermaziDocumento439 páginasImaging of Kidney Cancer - GuermaziNar RungrojanarakAinda não há avaliações
- Efficacy of Doctorvox On Mutational FalsettoDocumento8 páginasEfficacy of Doctorvox On Mutational FalsettoANA CRISTINA MENDEZ DIAZAinda não há avaliações
- AminoglycosidesDocumento20 páginasAminoglycosidesHassan.shehri100% (5)
- PN NCLEX - Integrated (A)Documento63 páginasPN NCLEX - Integrated (A)fairwoods89% (19)
- Nursing ShortageDocumento16 páginasNursing Shortageapi-240927368Ainda não há avaliações
- Brief Notes Parish of St. RafaelDocumento3 páginasBrief Notes Parish of St. RafaelAl F. Dela CruzAinda não há avaliações
- Aromatherapy - 600 Aromatherapy Recipes For Beauty, Health & Home - Plus Advice & Tips On How To Use Essential Oils - Nodrm PDFDocumento365 páginasAromatherapy - 600 Aromatherapy Recipes For Beauty, Health & Home - Plus Advice & Tips On How To Use Essential Oils - Nodrm PDFFernanda Rodriguez75% (4)
- Arcega ErlindaDocumento7 páginasArcega ErlindaIvonne TernidaAinda não há avaliações
- Retro VirDocumento3 páginasRetro VirJericho MangalinAinda não há avaliações
- ABC of Sexual Health: Taking A Sexual HistoryDocumento10 páginasABC of Sexual Health: Taking A Sexual HistoryCristina PerezAinda não há avaliações
- Cassey Ho - PIIT 2.0Documento45 páginasCassey Ho - PIIT 2.0Nikolett Mészáros100% (14)
- Rodríguez DinamometríaDocumento5 páginasRodríguez DinamometríaMariana Covarrubias SalazarAinda não há avaliações
- Rufenal EmulgelDocumento2 páginasRufenal EmulgelDr.2020Ainda não há avaliações
- Application For Life and Health Insurance ToDocumento5 páginasApplication For Life and Health Insurance Toimi_swimAinda não há avaliações
- Disability EssayDocumento7 páginasDisability Essayapi-459529771Ainda não há avaliações
- SBI3U Unit 1Documento5 páginasSBI3U Unit 1Sara SAinda não há avaliações
- Full Download Test Bank For Essentials of Genetics 8th Edition by Klug PDF Full ChapterDocumento36 páginasFull Download Test Bank For Essentials of Genetics 8th Edition by Klug PDF Full Chapterfencingvesper9dgb04100% (17)
- Sitogenetika Dan Peranannya Dalam Keganasan Hematologi: ResearchDocumento23 páginasSitogenetika Dan Peranannya Dalam Keganasan Hematologi: ResearchFebryanti Priskila SilaenAinda não há avaliações
- TOX-SICK by Suzanne Somers - ExcerptDocumento19 páginasTOX-SICK by Suzanne Somers - ExcerptCrown Publishing Group100% (1)
- Winter 2010 Natural FarmerDocumento48 páginasWinter 2010 Natural FarmerV1xWqAinda não há avaliações