Você também pode gostar
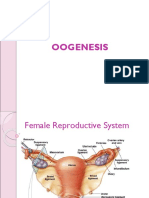
- Female Reproductive System-SsDocumento49 páginasFemale Reproductive System-SsJefri SandikaAinda não há avaliações
- Long Acting Contraceptive Contents of Progesterone HormoneDocumento34 páginasLong Acting Contraceptive Contents of Progesterone HormoneJefri SandikaAinda não há avaliações
- Growth at Puberty: Supplement ArticleDocumento9 páginasGrowth at Puberty: Supplement ArticleJefri SandikaAinda não há avaliações
- Uterostimulant and Relaxant 2Documento31 páginasUterostimulant and Relaxant 2Jefri SandikaAinda não há avaliações
- GTNDocumento58 páginasGTNJefri SandikaAinda não há avaliações
- The NeckDocumento36 páginasThe NeckJefri SandikaAinda não há avaliações
- Long Acting Contraceptive Contents of Progesterone HormoneDocumento34 páginasLong Acting Contraceptive Contents of Progesterone HormoneJefri SandikaAinda não há avaliações
- Oo GenesisDocumento21 páginasOo GenesisJefri SandikaAinda não há avaliações
- Psikologi LansiaDocumento29 páginasPsikologi LansiaJefri SandikaAinda não há avaliações
- The NeckDocumento36 páginasThe NeckJefri SandikaAinda não há avaliações
- The NeckDocumento36 páginasThe NeckJefri SandikaAinda não há avaliações
- Spermatogenesis and OogenesisDocumento23 páginasSpermatogenesis and OogenesisGerlJerl100% (1)
- Clinical Child Psychiatry, 2da KlykyloDocumento562 páginasClinical Child Psychiatry, 2da KlykyloAracelis Calzadilla Núñez100% (2)
- Female Reproductive System-SsDocumento49 páginasFemale Reproductive System-SsJefri SandikaAinda não há avaliações
- Silabus Entrepreneuship Revisi Baru 2 Sept 2015Documento5 páginasSilabus Entrepreneuship Revisi Baru 2 Sept 2015Jefri SandikaAinda não há avaliações
- Male Reproductive SystemDocumento42 páginasMale Reproductive SystemJefri SandikaAinda não há avaliações
- Opthalmia UmDocumento23 páginasOpthalmia Umnanu-jenuAinda não há avaliações
- 22acquired CataractDocumento16 páginas22acquired CataractJefri SandikaAinda não há avaliações
- Detection of Mutations Associated With Isoniazid and RifampinDocumento5 páginasDetection of Mutations Associated With Isoniazid and RifampinJefri SandikaAinda não há avaliações
- 1-Materi Anti Kanker Blok Obsfer-SKDKI - Dr. Asep SukoharDocumento68 páginas1-Materi Anti Kanker Blok Obsfer-SKDKI - Dr. Asep SukoharJefri SandikaAinda não há avaliações
- Error of Refraction - EditedDocumento43 páginasError of Refraction - EditedJefri SandikaAinda não há avaliações
- 3-Congestive Heart Failure-Dr AsepDocumento32 páginas3-Congestive Heart Failure-Dr AsepJefri SandikaAinda não há avaliações
- Ike Husen, Dwi Indria AnggrainiDocumento21 páginasIke Husen, Dwi Indria AnggrainiJefri SandikaAinda não há avaliações
- TB WWW - Nejm.org, Doi, PDF, 10.1056, NEJMra1200894Documento11 páginasTB WWW - Nejm.org, Doi, PDF, 10.1056, NEJMra1200894desiAinda não há avaliações
- Glands Associated With Digestive-SsDocumento30 páginasGlands Associated With Digestive-SsJefri SandikaAinda não há avaliações
- Cardiovascular PhysiologyDocumento43 páginasCardiovascular PhysiologyJefri SandikaAinda não há avaliações
- SISTEM IMUN Saluran PencernaanDocumento32 páginasSISTEM IMUN Saluran PencernaanJefri SandikaAinda não há avaliações
- TB WWW - Nejm.org, Doi, PDF, 10.1056, NEJMra1200894Documento11 páginasTB WWW - Nejm.org, Doi, PDF, 10.1056, NEJMra1200894desiAinda não há avaliações
- Cardiovascular PhysiologyDocumento43 páginasCardiovascular PhysiologyJefri SandikaAinda não há avaliações
- Surgery: BackgroundDocumento22 páginasSurgery: BackgroundJefri SandikaAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Polycystic Liver Disease A Case ReportDocumento5 páginasPolycystic Liver Disease A Case ReportEKO SANDY SINAGAAinda não há avaliações
- Renal Ultrasound Made Easy - Step-By-Step Guide - POCUS 101Documento45 páginasRenal Ultrasound Made Easy - Step-By-Step Guide - POCUS 101skype72214100% (2)
- Session #42 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Documento4 páginasSession #42 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Nicole Ken AgdanaAinda não há avaliações
- Diamond-Blackfan Anemia Is A DisorderDocumento22 páginasDiamond-Blackfan Anemia Is A DisorderDarem SoAinda não há avaliações
- Pathology Polycystic Kidney DiseaseDocumento4 páginasPathology Polycystic Kidney DiseaseOnyedika EgbujoAinda não há avaliações
- Nephrology by Prof NegoDocumento9 páginasNephrology by Prof NegoAbedinego MalukaAinda não há avaliações
- Renal UltrasoundDocumento179 páginasRenal UltrasoundJuhar AhamedAinda não há avaliações
- Autosomal Dominant Polycystic Kidney DiseaseDocumento11 páginasAutosomal Dominant Polycystic Kidney DiseaserutwickAinda não há avaliações
- CNN ExamDocumento167 páginasCNN ExamDiana Negron100% (7)
- Pathology - Chapter 20.2Documento6 páginasPathology - Chapter 20.2Cory GrayAinda não há avaliações
- Human Diseases 8th Edition Zelman Test BankDocumento15 páginasHuman Diseases 8th Edition Zelman Test Bankquatchristabelfa55hd100% (26)
- Journal Kidney StonesDocumento7 páginasJournal Kidney Stonesnelyang17Ainda não há avaliações
- Ploughing Through PACES Collected by DR Azmy PDFDocumento385 páginasPloughing Through PACES Collected by DR Azmy PDFtejbirsingh2013Ainda não há avaliações
- Imaging Vesika Seminalis Dan Vas DeferenDocumento68 páginasImaging Vesika Seminalis Dan Vas DeferenRivani KurniawanAinda não há avaliações
- Polycystic KidneyDocumento10 páginasPolycystic Kidneymanish dafdaAinda não há avaliações
- Renal Tumor and Polycystic Kidney DiseaseDocumento6 páginasRenal Tumor and Polycystic Kidney DiseaseMahdawwAinda não há avaliações
- 4th Year MBBS Final Test 2021 MCQ Paper With KeyDocumento9 páginas4th Year MBBS Final Test 2021 MCQ Paper With KeySaima IramAinda não há avaliações
- Cystic Diseases of The KidneyDocumento14 páginasCystic Diseases of The KidneyBarda GulanAinda não há avaliações
- Ginjal PolikistikDocumento6 páginasGinjal PolikistikNovi YudiaAinda não há avaliações
- Kidney DiseaseDocumento51 páginasKidney DiseaseRoland IntudAinda não há avaliações
- Autosomal Dominant DiseasesDocumento3 páginasAutosomal Dominant DiseasesAliHassanAinda não há avaliações
- Renal Pathology: Kidney and The Urinary Collecting SystemDocumento37 páginasRenal Pathology: Kidney and The Urinary Collecting Systemapplesncore100% (1)
- SOLVED Recalls April 2018 and PreviousDocumento256 páginasSOLVED Recalls April 2018 and PreviousNQ ZAinda não há avaliações
- Ciliopatias PDFDocumento11 páginasCiliopatias PDFsantiagoluna bAinda não há avaliações
- Gangguan Pada Ginjal Dan UreterDocumento127 páginasGangguan Pada Ginjal Dan UreterFebrina TrizaAinda não há avaliações
- Vichi Goel (Case of Polycystic Kidney Disease)Documento11 páginasVichi Goel (Case of Polycystic Kidney Disease)Hey ReelAinda não há avaliações
- CRF TextbookDocumento5 páginasCRF TextbookThirdie LacorteAinda não há avaliações
- Congenital AnomaliesDocumento94 páginasCongenital AnomaliesDeepti Kukreti100% (1)
- Master Pass 2021Documento248 páginasMaster Pass 2021Sama Diares100% (4)
- Essentials of Internal MedicineDocumento832 páginasEssentials of Internal MedicineEmanuelMC100% (75)