Você também pode gostar
- Fever and Rash Apcp 260818 FinalDocumento69 páginasFever and Rash Apcp 260818 FinalPriscilla Putri HarmanyAinda não há avaliações
- AppendicitiesDocumento58 páginasAppendicitiesGAURAV50% (2)
- PPT DIARHEA IN CHILDRENDocumento31 páginasPPT DIARHEA IN CHILDRENRifka AnisaAinda não há avaliações
- Recent Update in The Management of Invasive Fungal InfectionDocumento30 páginasRecent Update in The Management of Invasive Fungal Infectionanoop61100% (3)
- Diarrhea: WHO and IMCI GuidelinesDocumento37 páginasDiarrhea: WHO and IMCI GuidelinesJohn Christopher LucesAinda não há avaliações
- Approach To FeverDocumento80 páginasApproach To FeverRaditia AbrahamAinda não há avaliações
- Kuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)Documento17 páginasKuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)DillaAinda não há avaliações
- Problem-based Approach to Gastroenterology and HepatologyNo EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisAinda não há avaliações
- Atelectasis. Mechanisms, Diagnosis and Management (Peroni, 2000)Documento5 páginasAtelectasis. Mechanisms, Diagnosis and Management (Peroni, 2000)Renato Li SoldevillaAinda não há avaliações
- Adrenal DisordersDocumento32 páginasAdrenal DisordersJyoti ChadhaAinda não há avaliações
- A Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutNo EverandA Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutNota: 5 de 5 estrelas5/5 (1)
- Kuliah ADENOMYOSISDocumento38 páginasKuliah ADENOMYOSISmarajuuAinda não há avaliações
- Pediatric Normal ValueDocumento4 páginasPediatric Normal ValueyaniarsusinAinda não há avaliações
- Ventikular Septal Defect FixDocumento18 páginasVentikular Septal Defect FixPutri Sari DewiAinda não há avaliações
- Case AppendicitisDocumento30 páginasCase AppendicitisSarahAinda não há avaliações
- Asthma in the 21st Century: New Research AdvancesNo EverandAsthma in the 21st Century: New Research AdvancesRachel NadifAinda não há avaliações
- Children With Henoch Schonlein Purpura 2.0Documento13 páginasChildren With Henoch Schonlein Purpura 2.0soniaAinda não há avaliações
- Neurodermatitis (Lichen Simplex Chronic)Documento26 páginasNeurodermatitis (Lichen Simplex Chronic)Yusran Ady FitrahAinda não há avaliações
- 2 DHF InternaDocumento59 páginas2 DHF Internasaladass 2Ainda não há avaliações
- Fluid Managementuntuk Mahasiswa SajaDocumento56 páginasFluid Managementuntuk Mahasiswa SajaPratami Rieuwpassa IIAinda não há avaliações
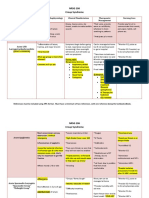
- NRSG 206 Croup SyndromeDocumento3 páginasNRSG 206 Croup SyndromeGirlwithnonameAinda não há avaliações
- Bacterial MeningitisDocumento1 páginaBacterial MeningitisDavid HylandAinda não há avaliações
- Special Sense System Group 6Documento24 páginasSpecial Sense System Group 6RushdaAinda não há avaliações
- Referat Kulit KakayDocumento26 páginasReferat Kulit KakayRezky Dwiputra FellanysAinda não há avaliações
- Congenital SyphilisDocumento3 páginasCongenital SyphilisadmusAinda não há avaliações
- Referat HDKDocumento29 páginasReferat HDKAga Haris100% (1)
- 194 Surgical Cases PDFDocumento160 páginas194 Surgical Cases PDFkint100% (4)
- MeningitisDocumento20 páginasMeningitisAmalia Tri UtamiAinda não há avaliações
- Arthritis, Suppurative Arthritis) : Pyogenic Arthritis (Septic Arthritis, InfectiveDocumento4 páginasArthritis, Suppurative Arthritis) : Pyogenic Arthritis (Septic Arthritis, InfectiveRajveerAinda não há avaliações
- Clinical Abstract TEMPLATEDocumento3 páginasClinical Abstract TEMPLATEDiannesa April GolosindaAinda não há avaliações
- Bartter SyndromeDocumento3 páginasBartter SyndromeEnny Andriani100% (1)
- Id ModuleDocumento4 páginasId ModuleKumar AdityaAinda não há avaliações
- Jurnal Reading MataDocumento37 páginasJurnal Reading MataAiya Auri GumantiAinda não há avaliações
- Anak 3.1 Infective Endocarditis DRTLTDocumento21 páginasAnak 3.1 Infective Endocarditis DRTLTAnastasia PinkyAinda não há avaliações
- Pola Imunologi Janin Dalam Kehamilan Dengan Toxoplasmosis: Khairunnisa Abd Rauf A.Zakaria Amien Octo ZulkarnainDocumento18 páginasPola Imunologi Janin Dalam Kehamilan Dengan Toxoplasmosis: Khairunnisa Abd Rauf A.Zakaria Amien Octo ZulkarnainArdian Zaka RAAinda não há avaliações
- Cerebral Palsy-GWC and DCF 2010Documento22 páginasCerebral Palsy-GWC and DCF 2010Jay SorianoAinda não há avaliações
- Approach To The Child With Anemia - UpToDateDocumento41 páginasApproach To The Child With Anemia - UpToDateDaniel Enrique CardenasAinda não há avaliações
- HepatosplenomegalyDocumento49 páginasHepatosplenomegalyTarun SinghAinda não há avaliações
- Japanese EncephalitisDocumento14 páginasJapanese EncephalitisMuhammad Rafli AkbarAinda não há avaliações
- Albendazole in PediatricsDocumento38 páginasAlbendazole in PediatricsKishore ChandkiAinda não há avaliações
- Walking Pneumonia, (Mycoplasma Pneumonia) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandWalking Pneumonia, (Mycoplasma Pneumonia) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Toxic Shock Syndrome - PPTX 1-1Documento49 páginasToxic Shock Syndrome - PPTX 1-1Mohammed Khedr100% (1)
- Ricardo A. Caicedo, MD: Pediatric Gastroenterology University of FloridaDocumento20 páginasRicardo A. Caicedo, MD: Pediatric Gastroenterology University of FloridaAsma SikanderAinda não há avaliações
- Diseases With The Rash Syndrome11.Documento33 páginasDiseases With The Rash Syndrome11.ManishAinda não há avaliações
- Approach To Child With WheezingpediatricsDocumento25 páginasApproach To Child With WheezingpediatricsshahinaAinda não há avaliações
- Ptl/Pprom and Multifetal Gestation: Anna Buabbud MD Ms3 LectureDocumento38 páginasPtl/Pprom and Multifetal Gestation: Anna Buabbud MD Ms3 LectureNik C0% (1)
- Respiratory Distress Syndrome: Islamic University Nursing CollegeDocumento21 páginasRespiratory Distress Syndrome: Islamic University Nursing Collegeyaumil agisnaAinda não há avaliações
- Kawasaki Disease LectureDocumento25 páginasKawasaki Disease LectureAlif ZainalAinda não há avaliações
- Gilut Herpes ZosteRDocumento24 páginasGilut Herpes ZosteRdimasahadiantoAinda não há avaliações
- Airway Management, Ventilation, and Oxygen TherapyDocumento56 páginasAirway Management, Ventilation, and Oxygen TherapybrentupdegraffAinda não há avaliações
- Critical Appraisal RCTDocumento7 páginasCritical Appraisal RCTAisya FikritamaAinda não há avaliações
- Lecture-4 Viral GastroenteritisDocumento37 páginasLecture-4 Viral GastroenteritislolitlolatAinda não há avaliações
- Management of Tuberculosis: A guide for clinicians (eBook edition)No EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Ainda não há avaliações
- Case ReportDocumento28 páginasCase Reportgraceswan100% (1)
- More Than A Sore ThroatDocumento17 páginasMore Than A Sore ThroatEmily EresumaAinda não há avaliações
- Batuk Kronik BerulangDocumento24 páginasBatuk Kronik BerulangHameldo Andika PattinasaranyAinda não há avaliações
- Brochure Selector Guide EN-web-protectedDocumento16 páginasBrochure Selector Guide EN-web-protectedPierre-Olivier MouthuyAinda não há avaliações
- The Manuals Com Cost Accounting by Matz and Usry 9th Edition Manual Ht4Documento2 páginasThe Manuals Com Cost Accounting by Matz and Usry 9th Edition Manual Ht4shoaib shakilAinda não há avaliações
- Ed A 02.00 I 01Documento39 páginasEd A 02.00 I 01Enrique BlancoAinda não há avaliações
- сестр главы9 PDFDocumento333 páginasсестр главы9 PDFYamikAinda não há avaliações
- Report Web AuditDocumento17 páginasReport Web Auditanupprakash36Ainda não há avaliações
- Abdukes App PaoerDocumento49 páginasAbdukes App PaoerAbdulkerim ReferaAinda não há avaliações
- 32 EM GreenTechDocumento45 páginas32 EM GreenTechMark Lester RealAinda não há avaliações
- City Marketing: Pengelolaan Kota Dan WilayahDocumento21 páginasCity Marketing: Pengelolaan Kota Dan WilayahDwi RahmawatiAinda não há avaliações
- Constitutional Law OutlineDocumento28 páginasConstitutional Law OutlineCasey HartwigAinda não há avaliações
- NMAT PRACTICE SET 0619 - Rationale - TEST D. ChemistryDocumento10 páginasNMAT PRACTICE SET 0619 - Rationale - TEST D. ChemistryMianella RosalesAinda não há avaliações
- Swot Analysis of PiramalDocumento5 páginasSwot Analysis of PiramalPalak NarangAinda não há avaliações
- Old Book Buy or SellDocumento41 páginasOld Book Buy or SellPallavi Pallu50% (4)
- Making Electric Vehicles ProfitableDocumento18 páginasMaking Electric Vehicles ProfitablevjslkumarAinda não há avaliações
- Natureview Case StudyDocumento3 páginasNatureview Case StudySheetal RaniAinda não há avaliações
- Case: Iridium LLC: Bhanu - Divya - Harsh - NamitaDocumento9 páginasCase: Iridium LLC: Bhanu - Divya - Harsh - NamitaHarsh AgrawalAinda não há avaliações
- Rockonomics: Book Non-Fiction US & Canada Crown Publishing (Ed. Roger Scholl) UK & Comm John Murray (Ed. Nick Davies)Documento2 páginasRockonomics: Book Non-Fiction US & Canada Crown Publishing (Ed. Roger Scholl) UK & Comm John Murray (Ed. Nick Davies)Natasha DanchevskaAinda não há avaliações
- Lpm2.1theoryDocumento85 páginasLpm2.1theoryvetprabu34Ainda não há avaliações
- Danmachi Volume 15Documento319 páginasDanmachi Volume 15Muhammad Fazrul Rahman100% (1)
- 2-Port Antenna Frequency Range Dual Polarization HPBW Adjust. Electr. DTDocumento5 páginas2-Port Antenna Frequency Range Dual Polarization HPBW Adjust. Electr. DTIbrahim JaberAinda não há avaliações
- Ventures Onsite Market Awards 22062023 64935868dDocumento163 páginasVentures Onsite Market Awards 22062023 64935868dhamzarababa21Ainda não há avaliações
- The Board-Management RelationshipDocumento32 páginasThe Board-Management RelationshipAlisha SthapitAinda não há avaliações
- Vocab Money HeistDocumento62 páginasVocab Money HeistCivil EngineeringAinda não há avaliações
- The Fat Cat Called PatDocumento12 páginasThe Fat Cat Called PatAlex ArroAinda não há avaliações
- The Til Pat YearsDocumento1 páginaThe Til Pat Yearsrajkumarvpost6508Ainda não há avaliações
- Back To School Proposal PDFDocumento2 páginasBack To School Proposal PDFkandekerefarooqAinda não há avaliações
- Create PDF Book App in Android Studio - Download Free PDF Book Source Code PDFDocumento6 páginasCreate PDF Book App in Android Studio - Download Free PDF Book Source Code PDFshafiq09090% (1)
- The Convergent Parallel DesignDocumento8 páginasThe Convergent Parallel Designghina88% (8)
- Student's Lab Pack: Preteens 02 11 Weeks CourseDocumento30 páginasStudent's Lab Pack: Preteens 02 11 Weeks CourseMi KaAinda não há avaliações
- Evolve Instagram Marketing Guide - From Zero To 10k PDFDocumento132 páginasEvolve Instagram Marketing Guide - From Zero To 10k PDFAnjit Malviya100% (2)
- Students Name - Kendrick Joel Fernandes ROLL NO. 8250 Semester Vi Subject - Turnaround Management Topic-Industrial SicknessDocumento15 páginasStudents Name - Kendrick Joel Fernandes ROLL NO. 8250 Semester Vi Subject - Turnaround Management Topic-Industrial SicknesskarenAinda não há avaliações